Healthy Aging Physical Therapy Monthly Blog
Understanding Apathy in PD: 10 Ways to Beat Apathy at Its Own Game
Discover why apathy in Parkinson's disease is not laziness, but a neurological symptom that changes how the brain calculates effort and reward. Learn the science behind Parkinson's-related apathy and 10 practical, evidence-informed strategies to overcome it and stay engaged in exercise, social activities, and daily life.
When I think about apathy, I picture my now 15-year-old daughter as a toddler. Back then, whenever I asked her to do something she didn't want to do, her response was almost always the same:
"Don't wanna."
Pick up your toys? Don't wanna.
Put on your shoes? Don't wanna.
Go to dance class and leave mom behind? Definitely don't wanna.
Fortunately, she eventually outgrew that stage. But when I think about apathy in Parkinson's disease, I often think about that same simple response — not because people with Parkinson's are acting like toddlers, and certainly not because they're being stubborn or difficult, but because from the brain's perspective, apathy can sometimes be just that simple.
The Parkinson's brain looks at an activity — even one that is important, meaningful, or enjoyable—and responds with a very quick internal calculation:
"Don't wanna."
The challenging part is that this isn't a response you can always reason with. When we don't understand apathy, we often default to motivational strategies that work for people without Parkinson's disease. We remind people that exercise is good for them. We tell them their physical therapist recommended it. We encourage them to try harder, stay active, or think positively. All of those statements are logical, and all of them may be true. Unfortunately, apathy is not a problem of logic.
Apathy is a neurobiological brain problem - and it is an incredibly common and consistent non-motor symptom of Parkinson’s Disease.
Because of that, apathy can create frustration for everyone involved. Care partners may feel ignored or dismissed. Adult children may worry that their parent is giving up. Healthcare providers can spend months educating someone about exercise, medication management, or healthy habits only to see little follow-through. Meanwhile, the person with Parkinson's often feels guilty, ashamed, or misunderstood because they know what they should be doing but struggle to get started.
The result is that everyone is working hard, but they're working against a barrier they don't fully understand.
The good news is that once we understand the neurobiology behind apathy — what it is, why it happens, and how Parkinson's changes the brain's motivation systems — we can start to work around it instead of against it. Understanding apathy gives us the KEYS to beating apathy at its own game.
What Is Apathy?
Apathy is one of the most common non-motor symptoms of Parkinson's disease, affecting an estimated 20–50% of people living with Parkinson's and becoming more common as the disease progresses. Despite how frequently it occurs, it is also one of the most misunderstood symptoms.
Apathy is often mistaken for laziness, depression, lack of effort, or lack of interest. In reality, it is none of those things.
While depression is characterized by sadness, hopelessness, or loss of pleasure, apathy is primarily a disorder of motivation and initiation. People with apathy often still care deeply about their families, hobbies, health, and future. They may want to exercise, attend social events, participate in therapy, or spend time with friends. The challenge is not that they don't care. The challenge is that turning intention into action has become significantly harder.
One of the most helpful ways to understand apathy is to think of it like a Reward vs. Effort Seesaw.
In a healthy brain, the anticipated reward of an activity generally outweighs the effort required to do it. The brain looks at an activity and thinks, "Going for a walk will feel good," or "I'll enjoy seeing my friends," or "Exercise is worth the effort." The reward side of the seesaw stays high, making it easier to get started.
Parkinson's disease can alter that internal cost-benefit calculation. Researchers increasingly believe that apathy reflects changes within the brain's motivation circuits, many of which rely on dopamine and related neurotransmitter systems. As those circuits change, the brain begins to overestimate effort and underestimate reward. The seesaw flips. Activities that once felt worthwhile now feel burdensome before they've even begun.
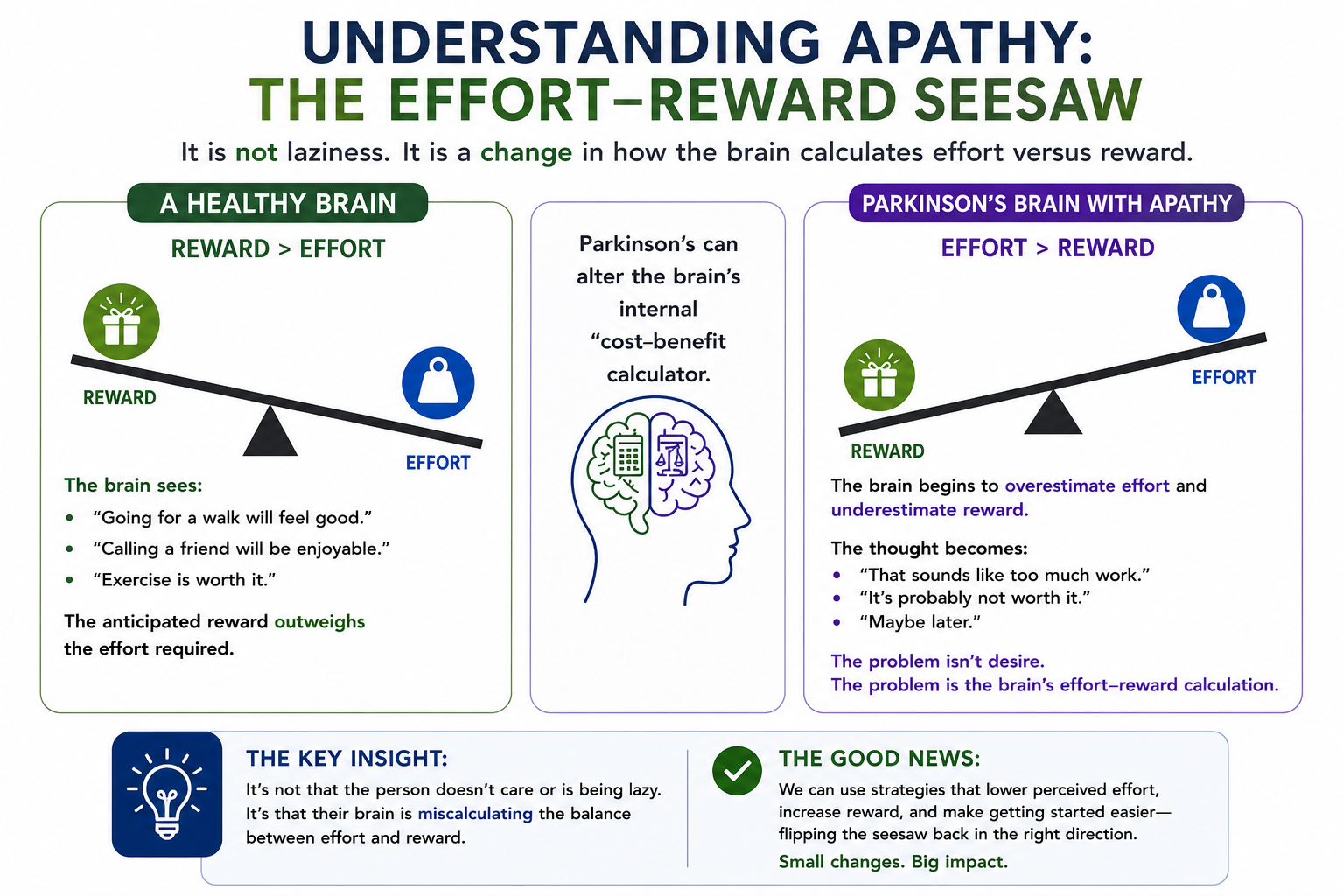
The internal dialogue becomes:
That sounds like a lot of work.
It's probably not worth it.
Maybe later.
Don't wanna.
What's fascinating is that many people with Parkinson's report feeling better after they exercise, attend a class, go for a walk, or meet up with friends. The activity itself wasn't the problem. The challenge was overcoming the brain's initial effort-reward calculation and getting started in the first place.
This understanding is important because it shifts our approach from trying to convince people to be motivated to creating systems that make action easier.
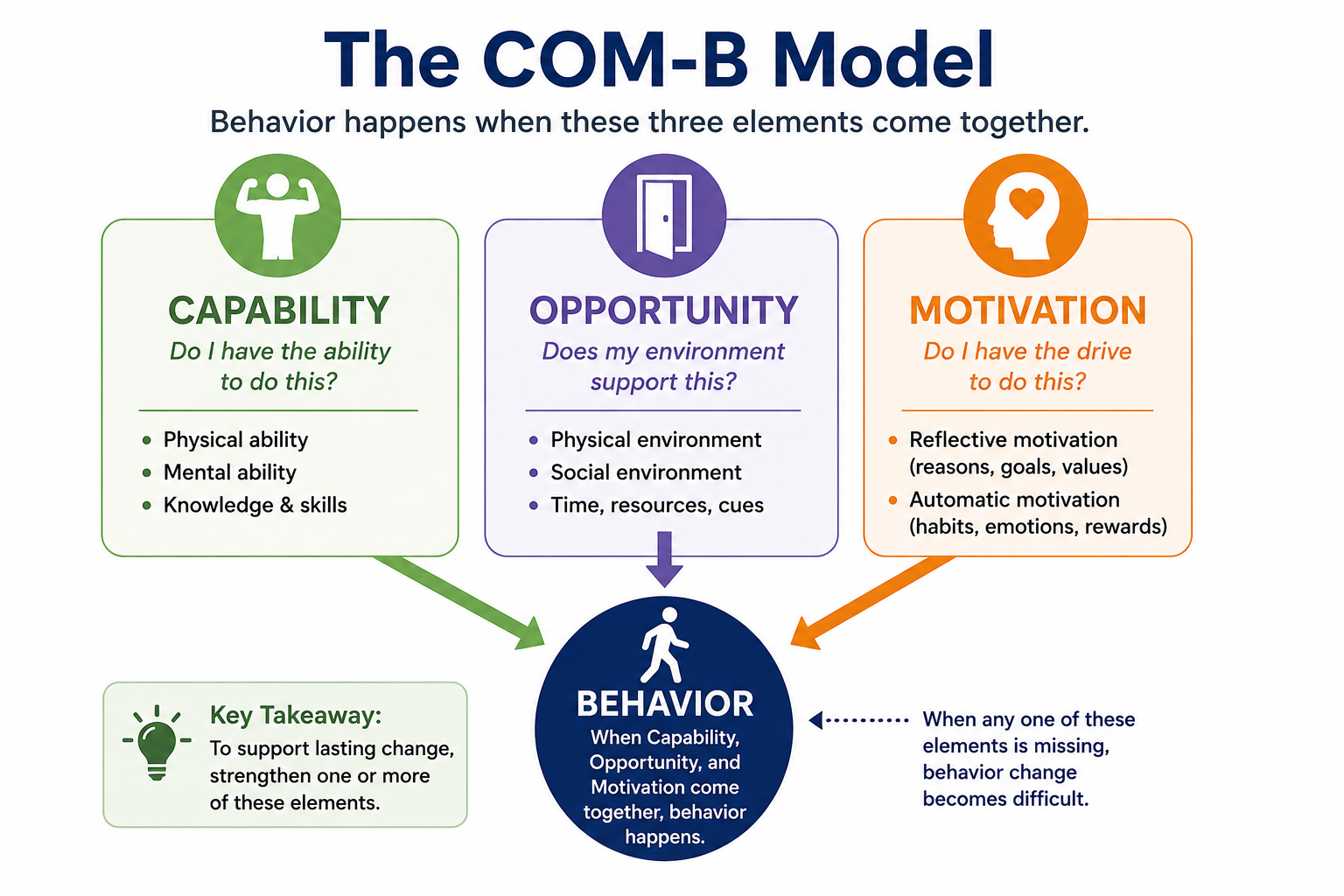
Using the COM-B Model to Outsmart Apathy
One of the most useful behavior-change frameworks discussed at the World Parkinson Congress was the COM-B Model. COM-B proposes that behavior occurs when three things come together:
Capability – Do I have the physical and cognitive ability to do this?
Opportunity – Does my environment support this behavior?
Motivation – Do I have enough drive, reward, habit, or reason to act?
When apathy is present, motivation is often the most obvious barrier, but it's rarely the only one. Sometimes the behavior is physically too difficult. Sometimes the environment creates unnecessary obstacles. Sometimes the reward feels too distant or too small to justify the effort.
The encouraging part is that we don't always have to increase motivation directly. In fact, trying to "motivate" someone with Parkinson's-related apathy is often the least effective approach. Instead, we can change the environment, simplify the task, build routines, leverage social support, and reconnect the activity to something meaningful. We can start to beat apathy at its own game! The following strategies are designed to do exactly that.
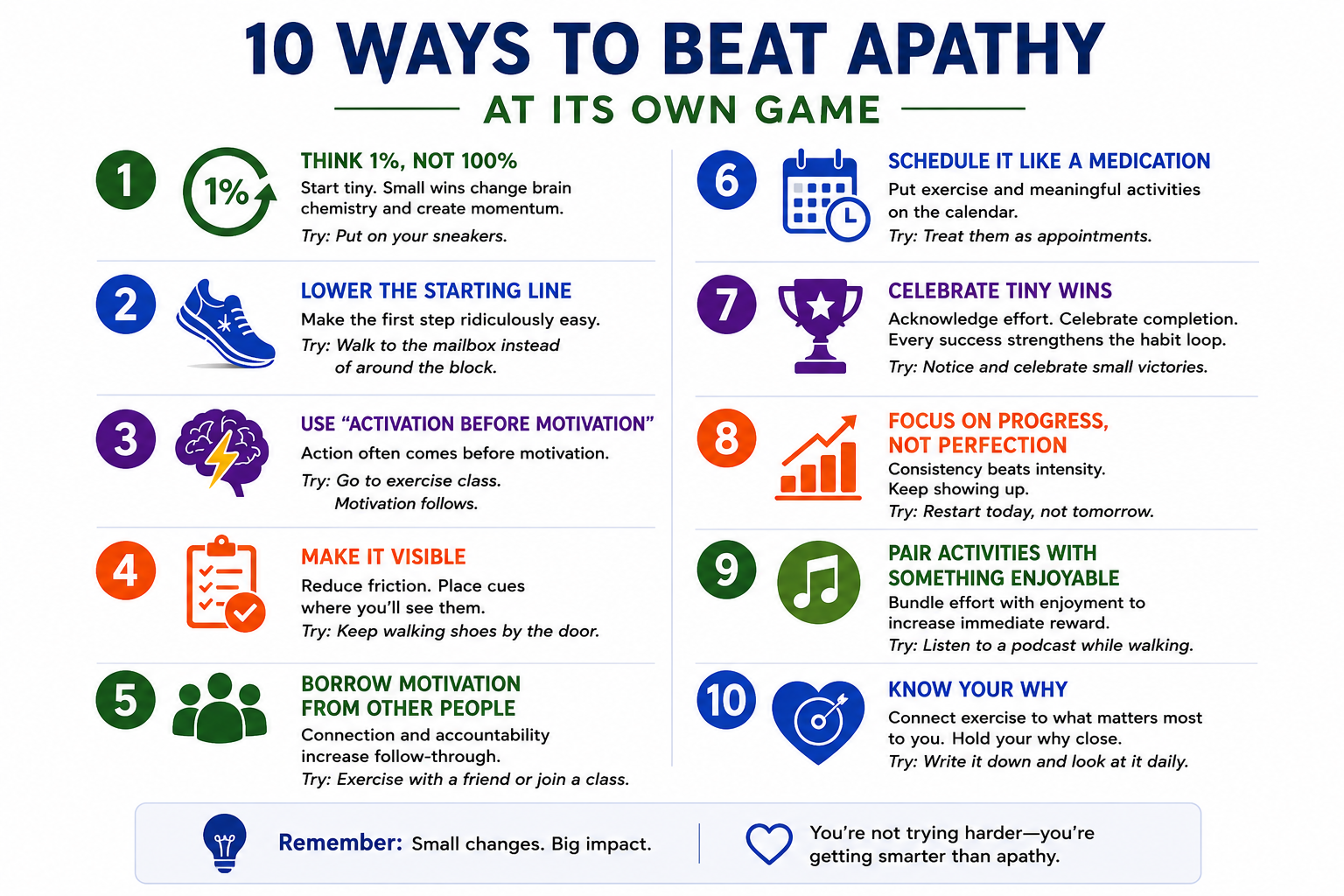
1. Think 1%, Not 100%
One of the most common mistakes people make is trying to change everything at once. Someone who hasn't exercised in months decides they're going to start walking 30 minutes every day. Someone who struggles with household tasks creates a long to-do list. Someone who wants to improve their health commits to changing their entire lifestyle overnight.
The Parkinson's brain often looks at those goals and immediately calculates the effort required. The result is predictable:
"Don't wanna."
Instead of focusing on the final destination, focus on the smallest possible first step. James Clear, author of Atomic Habits, calls this becoming "the type of person who shows up." The goal isn't to complete the workout. The goal is to begin.
For example, instead of committing to a 30-minute walk, commit to putting on your sneakers. Instead of promising yourself you'll complete your entire exercise program, commit to doing one exercise. Instead of attending an hour-long support group, commit to walking through the door. When I go running (which in case you're wondering my brain shouts loudly ‘Don’t wanna!!!), I give myself mini-goals - I’m not out there to run 3 miles, but I am going to run to the next driveway.
The beauty of small actions is that they dramatically reduce perceived effort while creating momentum. Often the hardest part isn't the activity itself—it's getting started.
COM-B Target: Opportunity and Motivation
2. Lower the Starting Line
Closely related to the 1% rule is the idea of lowering the starting line. We tend to believe success comes from raising expectations. In reality, success often comes from making the first step easier.
Many people with Parkinson's create goals that are so ambitious they become intimidating. The brain sees a mountain and decides it would rather stay on the couch.
Lowering the starting line means creating a version of success that feels almost impossible to fail.
If your goal is strength training, perhaps success today is one set of sit-to-stands.
If your goal is walking, perhaps success is walking to the mailbox.
If your goal is exercising three times this week, perhaps success is getting dressed in your exercise clothes and going to check out the local gym or observing a local PD fitness class.
The goal isn't to stay there forever. The goal is to create enough forward momentum that the next step becomes easier.
COM-B Target: Capability and Opportunity
3. Use Activation Before Motivation
Many people believe motivation comes first and action follows, but research suggests the opposite is often true. We wait to feel motivated before exercising. We wait to feel inspired before starting a project. We wait to feel energetic before going out with friends.
The problem is that motivation is unreliable.
Behavioral science consistently shows that action often creates motivation rather than the other way around. Once we begin moving, the brain receives new information. The activity may be enjoyable. We may feel accomplished. We may realize the task wasn't nearly as difficult as anticipated.
For someone with Parkinson's, this is a powerful concept because it shifts the goal from "feel motivated" to "take one action."
You don't have to want to go to exercise class.
You just have to get in the car.
COM-B Target: Motivation
4. Make It Visible
One of the easiest ways to improve follow-through is to redesign your environment.
The more effort required to remember a behavior, the less likely it is to happen. This becomes particularly important in Parkinson's disease, where cognitive load may already be increased. Think about your daily environment.
Do your walking shoes live in the back of a closet?
Are your exercise bands buried in a drawer?
Do you have to search for your water bottle every morning?
Every additional step increases friction.
Instead, place cues where you'll see them. Leave your walking shoes by the door. Keep exercise equipment near your favorite chair. Put your medication organizer somewhere visible. Use calendars, reminders, and visual prompts.
Successful habits often depend less on willpower and more on environment.
COM-B Target: Opportunity
5. Borrow Motivation From Other People
One of the strongest findings in Parkinson's exercise research is that people tend to do better when they're connected to others. Humans are social creatures and we are far more likely to show up when someone else is expecting us.
A walking partner creates accountability.
An exercise class creates routine.
A support group creates connection.
A personal trainer creates structure.
Social support also provides something equally important: encouragement during the inevitable periods when motivation is low. There will be days when you don't feel like exercising. There will be days when symptoms are frustrating. Having people around you who understand those challenges can make all the difference.
Sometimes we don't need more motivation.
Sometimes we just need good company.
COM-B Target: Opportunity and Motivation
6. Schedule It Like a Medication
Most people don't wake up each morning and ask themselves whether they feel motivated to take their medication - They simply do it.
Exercise and meaningful activities deserve the same level of commitment.
One of the most effective strategies for overcoming apathy is removing the decision altogether. Rather than deciding each day whether you'll exercise, decide once and put it on the calendar.
Monday at 10:00 AM.
Wednesday at 10:00 AM.
Friday at 10:00 AM.
Done.
Every decision requires energy. Every decision creates an opportunity for the Parkinson's brain to say "maybe later." Scheduling turns exercise from a choice into a routine.
COM-B Target: Opportunity
7. Celebrate Tiny Wins
The Parkinson's brain can become very good at focusing on what's missing.
"I only walked ten minutes."
"I didn't finish everything."
"I should have done more."
Unfortunately, this mindset reduces reward and reinforces apathy. Behavioral science teaches us that behaviors that get rewarded tend to get repeated. The reward doesn't need to be large. It simply needs to exist.
Did you exercise today? Celebrate it.
Did you attend your support group? Celebrate it.
Did you do one exercise instead of none? Celebrate it.
Your celebration can be a physical ‘air-five’ to yourself, a verbalized ‘You did great today! or a check-off on your tracking worksheet. Progress is progress and repeated acknowledgement of your success will help reset your reward vs. effort seesaw in the proper direction.
Tiny wins create momentum, confidence, and a stronger sense of self-efficacy.
COM-B Target: Motivation
8. Focus on Progress, Not Perfection
Perfectionism can be surprisingly damaging.
When people believe success means doing everything perfectly, they often choose not to start at all.
Missed one workout? The week feels ruined.
Missed a few days? The month feels ruined.
Behavior change doesn't work that way.
The people who succeed long-term aren't the people who never miss a day. They're the people who recover quickly when they do.
One missed workout doesn't matter.
One missed week doesn't matter.
What matters is returning.
Apathy loves all-or-nothing thinking. Progress thrives on flexibility. Instead of letting one missed opportunity derail the next, adopt a ‘next best decision’ mindset and take focus forward, not behind you.
COM-B Target: Motivation
9. Pair Activities With Something Enjoyable
Researchers sometimes call this "temptation bundling."
The idea is simple: combine something you need to do with something you enjoy doing to help increase the immediate reward associated with the activity.
Try listening to your favorite podcast while walking or saving your favorite television show for while you ride your riding the stationary bike.
Make a plan to meet a friend for coffee after exercise class.
The Parkinson's brain often discounts future rewards. Pairing an activity with something enjoyable helps bring some of that reward into the present moment.
COM-B Target: Motivation
10. Know Your Why
This may be the most important strategy of all.
People don't stay motivated because of exercise - they stay motivated because of what exercise allows them to do. If you ask most people why they exercise, most will answer something like ‘I know it’s good for me’ or ‘my doctor said to’ but that's not a why - that's an instruction.
A real why needs to be much more personal.
Maybe it's so you can keep attending your granddaughter's soccer games, or walk on the beach during your annual family vacation.
Maybe it's so you can keep traveling, gardening or playing pickleball with your friends
Maybe it's dancing at a wedding - or being able to walk your daughter down the aisle.
Maybe it's remaining independent and continuing to live in your own home.
THESE are reasons worth fighting for.
When symptoms are challenging and motivation is low, your why becomes an anchor. It reminds you that exercise isn't really about exercise. It's about protecting the life you want to continue living.
Write your why down.
Put it on the refrigerator.
Keep it in your wallet.
Talk about it with your family.
And when the Parkinson's brain says "don't wanna," remind yourself why you started in the first place.
Hold your why tight.
The Bottom Line
Apathy lies.
It tells you the effort is too great. It tells you it isn't worth it. It tells you you'll do it tomorrow, but the science tells a different story.
Most people feel better after they start.
Most people discover the activity wasn't nearly as difficult as their brain predicted.
And most people find that small actions, repeated consistently over time, can create remarkable changes in strength, mobility, confidence, independence, and quality of life.
The goal isn't to overpower apathy through sheer willpower. The goal is to understand how Parkinson's changes the brain's effort vs. reward calculation and then build systems that make action easier.
Start small.
Make it visible.
Use support.
Know your why.
And remember: sometimes beating apathy isn't about trying harder.
It's about outsmarting it and beating it at its own game. And PS: If your brain responded ‘don’t wanna’ after reading all 10 of these tips, it’s because 10 tips is too much right now. Follow the 1% rule and pick ONE TIP and start there. I promise it will help.

Parkinsonisms: What Parkinson’s Is… and What It Isn’t
Learn the key differences between Parkinson’s disease and atypical Parkinsonism syndromes like PSP, MSA, Lewy Body Dementia, and CBD—and how diagnosis and rehabilitation approaches differ.
Written by: Dr. Katie Wadland, PT, DPT, Board-Certified Geriatric Clinical Specialist, Owner of Healthy Aging PT
When most people hear “Parkinson’s disease,” they picture a very specific condition—and for many, that’s accurate. But in our work at Healthy Aging Physical Therapy, we often meet patients whose symptoms look like Parkinson’s… but don’t quite follow the same rules.
These are called Atypical Parkinsonism syndromes, or simply Parkinsonisms.
As a Parkinson’s specialty practice, we’ve had the unique opportunity to work closely with individuals living with conditions like Lewy Body Dementia (LBD), Progressive Supranuclear Palsy (PSP), Multiple System Atrophy (MSA) and Corticobasilar Degernation (CBD). These diagnoses are less common - but incredibly important to recognize, as while there is overlap with Parkinson’s disease, the rehabilitation approach must be thoughtfully adapted for each condition.
Let’s break it down.
What Are “Parkinsonisms”?
“Parkinsonism” is a term used to describe a group of neurological conditions that share key movement features seen in Parkinson’s disease, such as:
Slowness of movement (bradykinesia)
Stiffness (rigidity)
Balance and gait difficulties
However, these conditions have different underlying causes, faster progression, and often respond differently (or poorly) to typical Parkinson’s medications like levodopa.
How Are Parkinsonisms Diagnosed?
Diagnosis can be challenging and often evolves over time. Often, someone is initially diagnosed with Parkinson’s Disease, but when symptom progression is different than expected, or the individual does not respond to medications as expected, an atypical form may be suspected. Other signs might include:
Early balance impairment or falls
Cognitive or autonomic changes early in the disease course
Eye movement abnormalities (especially in PSP)
Imaging and neurological exam findings
In many cases, diagnosis is clinical and may take time, as symptoms unfold and patterns become clearer. Fortunately, we now have more concrete ways to differentiate between the different syndromes including DAT Scans and Skin Biopsies:
DAT Scans: A DaTscan is a specialized imaging test that looks at dopamine activity in the brain. By looking at the patterns, doctors can now better identify if symptoms are coming from a neurodegenerative cause, like Parkinson’s Disease or an Atypical Parkinson’s Syndrome, or from something else, like Essential Tremor or drug-induced symptoms. It is important to be aware a DAT Scan can NOT differentiate between idiopathic Parkinson’s and Atypical Parkinson’s Disease.
Skin Biopsies: A skin biopsy can be taken and analyzed for abnormal alpha-synuculein deposits. When these are identified in the sample, it can help differentiate between the idiopathic form of Parkinson’s and some of the atypical forms of the disease. It is important to note that while it can differentiate the two from one another, it can NOT identify which Atypical Parkinson’s disease a person may have.
As you can see, while we have many more tools at our disposal for proper diagnosis of Parkinson’s Disease and Atypical Parkinsonisms, it still remains a largely clinical diagnosis based on symptoms, progression of disease and response to medication treatment.
What are the Different Atypical Parkinson’s Diseases?
Lewy body Dementia (LBD)
Lewy Body Dementia is a neurodegenerative condition characterized by a combination of:
Cognitive impairment
Parkinsonian motor symptoms
Fluctuations in alertness
Visual hallucinations
What Makes It Different Than Parkinson’s?
Cognition is affected early, often before or alongside movement symptoms
Fluctuating attention and alertness (good days and bad days are common - and presentation may even within throughout the day)
Visual hallucinations are common
Patients may be sensitive to certain medications
How Is Rehab Different?
Rehabilitation for LBD requires a flexible, patient-centered approach:
Session-to-session variability is expected. Therapists must be prepared to adjust treatments, as needed, in real time.
Patients do best when care is focused on routine, familiarity, and caregiver involvement.
Due to the cognitive challenges, communication should be clear, calm and simple.
Balance and mobility training are still essential, but, patients may may need shorter sessions or breaks and should focus should focus more on compensatory strategies as it will be harder for patients to carryover instructions from session to session.
Progressive Supranuclear Palsy (PSP)
PSP is a neurodegenerative condition that affects:
Balance and walking
Eye movements (especially looking down)
Postural control (and most notably, results in retropulsion, or the sensation of falling backwards)
Spinal mobility (rigidity is a marked feature in people with PSP)
What Makes It Different Than Parkinson’s?
Early and frequent falls, often backward
Difficulty with vertical eye movements, especially downward gaze
Speech and swallowing issues tend to appear earlier
Minimal response to Parkinson’s medications
Axial rigidity (stiffness in the trunk more than limbs)
How Is Rehab Different?
Rehabilitation for PSP is very focused on safety and proactive management of symptoms:
Fall prevention is a #1 priority. This often involves prescribing an appropriate assistive device (we love the USTEP for our patients with PSP!), making changes to the home to make it safer and making recommendations for adequate supervision and teaching caregivers the skills they need to help their loved one move safely.
Therapists should assess and treat ocular coordination impairments. When patients can’t look down well, this impacts depth perception and fields of vision, making things like using stairs, curbs and navigating uneven terrain more difficult. People with PSP benefit from working on compensatory skills like visual scanning, and also on using visual exercises to maintain the ocular control they have.
Because of the areas impacted by PSP, people with PSP will have a more difficult time improving balance reactions and walking. They frequently do better with use of external cuing, like using targets on the floor or a laser, or by putting signs up throughout the home to remind them to use safe strategies like pushing off the chair to stand up, or holding on to a surface for support before reaching for something.
It is critical for someone with PSP to get therapy early! Progression of PSP is faster than in typical Parkinson’s Disease and the earlier we can address emerging changes and new symptoms, the more impact we can have on safety and quality of life.
Multiple Systems Atrophy (MSA)
MSA is a progressive neurological condition that affects:
Movement (Parkinsonian features)
Posture (more rounded, head-down positions)
Autonomic Nervous System (causing changes in blood pressure, bladder control and breathing)
What Makes It Different Than Parkinson’s?
Significant autonomic dysfunction causing frequent low blood pressure and syncope (passing out)
Bowel and bladder dysfunction is more common
Progression is faster than in typical Parkinson’s Disease
Minimal response to Parkinson’s medications
May also include cerebellar features like coordination issues
How Is Rehab Different?
Rehabilitation for MSA is requires careful monitoring and management of blood pressure in particular:
Vital sign monitoring should be completed before and during sessions and sessions may need to be modified to keep blood pressure in safe ranges.
Education should focus on strategies to maintain blood pressure in safe ranges throughout the day. This often requires a combination of medication management and coordination with doctors, and education for the patient and caregivers for using things like compression stockings or abdominal binders to help keep blood pressure high enough when they stand up.
Because orthostatic hypotension is common in MSA (drops in blood pressure with standing), it is important to include a seated warm up and slow progression to standing and walking activities during sessions.
Hydration is critical for patients with MSA. Being dehydrated will make the autonomic dysregulation worse and is a frequent cause of falls and hospitalizations for these patients.
Corticobasilar Degeneration (CBD)
CBD Corticobasal Degeneration (CBD) is a rare neurodegenerative condition that affects both the cortex (brain) and the basal ganglia, leading to a combination of movement and higher-level motor planning difficulties. It often presents asymmetrically, meaning one side of the body is significantly more affected than the other.
What Makes It Different Than Parkinson’s?
CBD has several unique features that sets it apart:
Marked asymmetry with one side affected more than the other
Apraxia is a key feature, which is difficulty performing purposeful or functional movements with a limb despite having the strength and motor control to do so
‘Alien Limb’ phenomenon is common - an arm or leg may seem to move involuntarily or feel disconnected from the body
Cortical sensory deficits make it difficult to interpret sensory information
Myoclonus is often present which looks like jerky or uncontrolled movements
Minimal to no response to Parkinson’s medications
Unlike Parkinson’s disease, where movement is primarily limited by slowness and rigidity, CBD involves a breakdown in motor planning and control at a higher neurological level.
How Is Rehab Different?
Rehabilitation for CBD Rehabilitation for CBD requires a shift in approach from “strength and movement” to motor planning, task breakdown, and functional adaptation:
Therapy should focus on task-specific training, and patients do best when breaking down movements into smaller, step-by-step components
Cuing should incorporate external cues, hand-over-hand support and modeling or demonstration as interpretation of body-based or sensory-cues will be very hard to understand
Compensation with the less affected side is critical to maintaining independence as long as possible
Consider use of adaptive strategies and equipment early on so training can be incorporated while motor control and cognition is at it’s best.
The Big Picture: Similar…But Not the Same
While all Parkinsonisms share common movement challenges, the differences between them matter—a lot. In Parkinson’s disease, we typically see a slower progression, a good response to medication (especially early on), and a rehabilitation approach that emphasizes amplitude, intensity, and long-term maintenance. In contrast, atypical Parkinsonisms often present with a faster or more complex progression and a more limited response to medication. Because of this, rehabilitation must shift—becoming more adaptive, more preventative, more caregiver-inclusive, and more medically integrated to address the broader range of symptoms these conditions can bring.
Hopefully this information has helped you better understand some of the key differences between typical, or idiopathic, Parkinson’s disease and the atypical forms of Parkinsonism. Whether you are a patient, caregiver, or therapist reading this, it is critical to recognize these differences—not only to advocate for an accurate diagnosis if things “just don’t feel right,” but also to find providers who understand these conditions and can truly individualize care.

Cutting Through the Chaos: Creating Effective Frameworks for Complex Patients
Many older adults don’t fit neatly into a single diagnosis—and neither does their care. In Cutting Through the Chaos: Creating Effective Frameworks for Working with Complex Patients, Dr. Katie Wadland, PT, DPT, Board-Certified Geriatric Clinical Specialist, shares how Healthy Aging Physical Therapy helps clinicians and families navigate the challenges of treating medically complex patients. Learn how to identify priorities, layer support, and build collaborative care plans that promote safety, independence, and resilience for older adults with multiple conditions.
Written by: Dr. Katie Wadland, PT, DPT, Board-Certified Geriatric Clinical Specialist Owner: Healthy Aging Physical Therapy
If you’ve ever worked with, or been, a patient who seems to have more going on that meets the eye, you know how challenging it can be. Fortunately, these are also often the most rewarding patients - and, most importantly, the ones who need us most.
At Healthy Aging Physical Therapy, our team specializes in exactly that: caring for complex patients—people with multiple diagnoses, long medical histories, and functional challenges who often feel like no one knows where to start. They’re the ones who have seen five other therapists, have a dozen specialists, and still feel stuck.

Why Our Patients Are So Complex
When you’re in physical or occupational therapy school, you learn about impairments in isolation.
A hip fracture? You study how to rebuild strength and balance.
A cardiac patient? You learn to monitor vitals and improve endurance.
A neurological condition? You focus on motor control, coordination, and safety.
But real-world patients with geriatric, neurologic, and complex medical needs don’t fit in tidy boxes. The people we serve are living with multiple comorbidities, often taking many medications, and facing social and emotional challenges that go far beyond their diagnosis list.
For example, many of our patients with Parkinson’s disease also experience osteoarthritis, chronic pain, memory loss, anxiety, and depression - and often have a partner who is also aging and managing their own medical issues to boot. Similarly, a patient referred for “hip fracture” is rarely just an orthopedic case. The fracture may have resulted from a fall, which stemmed from a combination of weakness, balance impairments, cardiac symptoms, and home safety challenges. Many live alone, with limited support and a history of sedentary behavior.
It’s no wonder that walking into these homes for an evaluation can feel overwhelming, even for seasoned clinicians.
Many of these individuals have already been discharged from other settings because progress stalled, the situation was too complicated, or insurance coverage ran out. Over time, we’ve become the go-to practice for these patients—the ones other providers refer when they aren’t sure what else to do. In many cases, we become the last stop—the “hail Mary” for patients who are exhausted from circling through the healthcare system.
So, how do we help?
Our Framework for Treating Complex Patients
Through experience and teamwork, we’ve developed a simple, realistic framework that helps our clinicians navigate these challenging situations - one that keeps both patient and therapist grounded, hopeful, and effective.
Whether you’re a therapist reading this, a patient with a complex background, or a caregiver trying to support a loved one, I hope these strategies help you cut through the chaos and find a starting point that leads to progress.
1. Focus on What Matters Most and Not Everything at Once
When faced with a dozen problems, it’s natural to want to fix them all. But that’s a recipe for overwhelm, and, inevitably, an ineffective therapeutic approach.
Instead, we teach our therapists to start by asking:
“What are the top one or two things we can help with right now that will most improve this person’s quality of life, safety, and independence?”
Sometimes that means addressing strength, balance, or mobility. Other times, it’s about helping the patient move again after weeks (or months) of fear and inactivity. Sedentary behavior, whether from pain, fear, or fatigue, triggers a cascade of physical and emotional decline and often, interrupting this cycle can be an important first step. Even small steps toward safe, confident movement can change everything. Sometimes, a compensatory approach is the right starting point: helping a patient obtain the proper wheelchair, walker, or other durable medical equipment to restore access to their home and community.
Time after time, we’ve learned that small wins matter. They build trust, confidence, and momentum - all critical ingredients for rapport and long-term success.
2. Layer in Support
We remind our team (and ourselves) that we can’t fix everything - and that’s okay. Somethings aren’t ‘fixable’ and other things are outside of our scope and capabilities.
Our role is to make a meaningful difference where we can, while also building a web of support around the patient to provide support for ‘the other things’. That often means:
Connecting patients with mental health providers when mood disorders or anxiety is a barrier
Coordinating with care team physicians and pharmacists to address medication-related issues
Referring our patients to trusted home health aides, elder services, or aging life-care specialists
Providing resources for community programs, support groups, and case managers
It’s not about doing it all ourselves - it’s about building the right team around each patient, one layer at a time.
3. Collaboration Is Key
When you work with a Healthy Aging therapist, you may only see one person walk through your door—but behind that therapist is an entire network of expertise.
Our team includes specialists in neurology, orthopedics, geriatrics, vestibular therapy, and cardiopulmonary rehab. We collaborate behind the scenes through discussion boards, case consults, and joint visits - bringing fresh ideas, new eyes and diverse perspectives to every complex case. Sometimes that collaboration means I’ll step in for a Complex Case Visit, working alongside the treating therapist to strategize solutions. Other times, the team shares insights online, helping each other troubleshoot mobility challenges, medication effects, or behavioral barriers.
That culture of teamwork is one of our greatest strengths—and one of the biggest reasons I feel our patients make progress where others have stalled.
4. Think Long-Term
Complex patients rarely fit neatly into a six-week plan of care. Their needs evolve, new issues arise, and maintaining stability often becomes the goal as much as improvement.
That’s why we emphasize continuity - treating each patient as someone we’ll likely know for years. When a patient is ready to discharge, we make sure:
A comprehensive post-discharge home program is in place
The patient has been connected with the appropriate community and medical supports
We have established a clear plan for future follow-up
For many, we transition them into a Maintenance Plan of Care under Medicare Part B, or into our Wellness program, Wellness365, where they continue to receive guided exercise and ongoing support to prevent decline.
Because our ultimate goal isn’t just short term rehab - it’s recovery and resilience.
What This Means for Patients and Families
If you’re a patient, caregiver, or family member feeling frustrated that “no one knows how to help,” please know: you’re not alone, and your situation isn’t hopeless.
Working with complex conditions takes time, teamwork, and the right perspective. The most important first step is finding professionals who know how to cut through the chaos - and, most importantly, who see you as a person first, not just a list of diagnoses, which is the heart of what we do at Healthy Aging Physical Therapy.

Wheelchairs 101: Understanding Wheelchair Options, Coverage and the Acquisition Process
Discover the options, coverage, and process involved in selecting the right wheelchair. From custom manual and power wheelchairs to scooters, learn how a well-matched chair can improve mobility, independence, and quality of life. Healthy Aging Physical Therapy offers in-home assessments to ensure your wheelchair fits your unique needs and living environment. Contact us today to start your journey to enhanced mobility!
Written By: Dr. Katie Wadland, PT, DPT, Board-Certified Geriatric Clinical Specialist
Owner: Healthy Aging Physical Therapy
As a physical therapist, I have had the privilege of working with many individuals who rely on wheelchairs to maintain their independence and quality of life. The reasons for needing a wheelchair are as diverse as wheelchair users themselves, and a well-matched chair can make a world of difference. From those with new spinal cord injuries who require an agile, lightweight manual chair to take the place of walking in the setting of traumatic paralysis, to the patient who has had a stroke and now needs a specialized ‘hemi-chair’ designed for propulsion with one side of the body, each journey is unique.
While many people initially see a wheelchair as a step back, I often see it as a step forward. A wheelchair can open doors to independence, freedom of mobility, and a reduced reliance on caregivers. Although I sometimes encounter hesitation or pushback when bringing up the idea of a wheelchair, I frequently find that once the process is complete, my patients experience newfound freedom and vastly improved quality of life.
In my current practice, I most often work with patients with neurodegenerative diseases, like multiple sclerosis (MS) or Parkinson’s Disease, who can still ambulate part of the time but may need a wheelchair with custom features, like the ability to tilt-in-space, elevate seat height or powered mobility, to manage fatigue, enable longer-distance mobility, support posture in the presence of kyphosis and scoliosis and maintain independence in their daily tasks. Most recently, I had the opportunity to help my own mother obtain a custom power wheelchair. After living with Parkinson’s disease (PD) for 20 years, her postural impairments began affecting her ability to breathe, function, and manage back pain. The chair provided her with much-needed relief and now allows her to access her facility’s dining room even during periods when walking is too difficult due to ‘off times’ and back pain.
(PS: You’ll see some pictures from my mom’s assessment and fitting throughout the blog - special thanks to Derek Logan, PT, ATP from REQ for your help with this process!)
No two reasons for needing a wheelchair are the same. This is why a thorough assessment by a knowledgeable therapist, in collaboration with a skilled vendor, is essential to finding the best solution for each individual’s needs. At Healthy Aging Physical Therapy, we frequently provide wheelchair assessment training in conjunction with a variety of local vendors and I’d like to take this opportunity to shed some light on what this typically entails.
Wheelchairs, Scooters and Powered Mobility Options
When it comes to mobility devices, there are many options to consider. The choice between a standard wheelchair, a custom manual or power chair, or a scooter depends on the user’s specific functional and medical needs. Each type of mobility aid comes with its own set of features, costs, and considerations.

Scooters
Scooters are three - or four-wheeled motorized devices for individuals who can sit upright and operate controls but require assistance for longer distances due to weakness or cardiopulmonary conditions. Scooters are an excellent choice for those with some mobility but who experience fatigue with walking. They are often not covered by insurance and usually require an out-of-pocket investment ranging from $800 to $3,000. Many scooters can break down or fold up for transportation and can be tried at local durable medical equipment vendors and pharmacies.
PS: The above image is from the movie Thelma. If you haven’t seen it yet, stop reading and go watch it:)

Transport Wheelchairs
Transport wheelchairs are often purchased online or at medical supply stores and are the lightest, most easily transportable wheelchairs available. They typically have small wheels and limited seat and lumbar support; this enables them to be light enough to transport easily in and out of the car, but are also not designed for long term use as they do not provide adequate postural support for the user. Transport wheelchairs are not typically covered by insurance (unless you meet the criteria for a standard chair, but cannot self-propel and have a 24/7 caregiver who can assist) and cost anywhere from $100-$300 typically.

Standard Manual Wheelchairs
Standard manual wheelchairs are the most basic option covered by insurance, and are often used for short-term needs or rental purposes. These chairs are manually propelled and typically cost between $100 and $500. They are ideal for individuals who do not require specialized features and need a temporary mobility solution. Medicare and other insurance plans may cover standard wheelchairs if they are deemed medically necessary, and are often issued during hospital stays in a ‘rent to own’ manner in which the Medicare beneficiary pays a small amount a month for thirteen months and then ‘owns’ the wheelchair.

Custom Manual Wheelchairs
Custom manual wheelchairs are tailored to the user’s specific dimensions and functional requirements. These chairs may include lightweight frames, adjustable seating, and positioning supports to enhance comfort and postural alignment. They are commonly used by individuals with conditions such as spinal cord injuries or neurological disorders. Custom manual wheelchairs generally cost between $1,500 and $5,000, depending on the materials and features. Custom manual wheelchair acquisition requires a wheelchair assessment by a therapist and vendor team, a visit with a doctor who will provide documentation to certify medical necessity, and insurance coverage often requires detailed documentation to justify the need for customization.
Power Wheelchairs
Power wheelchairs are motorized devices designed for individuals who have limited upper body strength or severe postural issues. These chairs can include advanced features such as recline, tilt-in-space, and elevation to address complex needs. Power wheelchairs are best suited for individuals with conditions like MS, Parkinson’s disease, or other impairments that significantly limit strength and mobility. The cost of a power wheelchair can range from $2,000 to over $20,000, depending on the level of customization and technology. Medicare typically covers power wheelchairs, but only after a thorough assessment to establish medical necessity. These assessments need to be provided by a therapist and vendor team, and the individual will also need to visit with their doctor who will need to complete additional paperwork (‘Face to Face’ visit) to support the medical necessity of this device.

Fun Fact: The average custom power chair weighs between 200 and 300 pounds. And, no, you cannot lift it into the trunk of your car!
Beyond Mobility: Other Important Reasons to Consider a Wheelchair
While mobility is often the primary reason for a wheelchair, there are several other important considerations that influence the need for a specific type of chair.

Preventing Skin Breakdown and Pressure Ulcers
For individuals who spend long hours in their wheelchairs, proper seating and support are critical to prevent skin breakdown and pressure ulcers. Specialized cushions, adjustable seat angles, and recline and tilt-in-space features can help individuals redistribute pressure and protect vulnerable areas, ensuring comfort and long-term skin health.
Providing Postural Support
Postural support is essential for individuals with trunk weakness or structural deformities. A well-designed wheelchair can enhance alignment, improving not only comfort but also critical functions like breathing and digestion. For example, we might choose to increase the seat angle (aka ‘seat dump’) and use a contoured seat back to improve pelvic alignment and maintain a healthy posture throughout the day, reducing pain and fatigue.
Enhancing Functional Abilities
Wheelchairs with advanced features can improve functional abilities in daily life. Elevating seat mechanisms, for instance, allow users to reach higher surfaces such as kitchen counters and cabinets, enabling tasks like cooking and cleaning. Additionally, alternative drive options like head controls or adapted joysticks can enable mobility even in users with limited hand function.
Reducing Caregiver Reliance
By addressing mobility and functional needs comprehensively, a wheelchair can reduce reliance on caregivers. This increased independence not only improves the user’s quality of life but also eases the burden on family members and care teams and can improve family dynamics considerably.

How do I get a Custom Wheelchair?
Acquiring the right wheelchair is a multi-step process that involves collaboration between the patient, therapist, and vendor. Here is what to expect:
Initial Wheelchair Assessment: Your therapist and vendor team will conduct a comprehensive assessment of the individual’s mobility, strength, posture, and functional needs. This evaluation helps determine the type of wheelchair that will best meet the user’s requirements. These can be done in a Wheelchair Clinic or at-home with a provider like Healthy Aging Physical Therapy. You will have the opportunity to trial a chair similar to the one you will likely end up with to see if it would be a good fit.
Therapist/Vendor Collaboration: The therapist works closely with the wheelchair vendor to determine the best type of wheelchair for you, and identifies any necessary modifications or adaptations to meet your needs. They then work together to fill out the necessary paperwork and complete a Letter of Medical Necessity.
Documentation Submission: The prescribing physician, therapist and vendor provide detailed paperwork, including the assessment findings and justification for medical necessity. This documentation is submitted to Medicare or other insurance providers for approval.
Approval and Order Placement: Once the paperwork is approved, the vendor places the order for the wheelchair. Once approved, the equipment is ordered and the wheelchair is prepared for you. For custom manual or power chairs, this step may involve further adjustments and fittings.
Delivery and Fitting: Once the wheelchair is ready, your vendor and therapist will meet with you again to deliver the chair and provide any additional modification that may be needed. Things like the arm rest height and head rest position will need to be set for you specificically to ensure the best fit. If there are any larger issues, your vendor may take pieces of the chair back to be adapted as needed.
Wheelchair Training: Now the fun begins! Just like learning to drive a car, learning to drive your new wheelchair will take some practice. Your therapist will work with you to learn to drive it forward, backwards and to turn so you can safely and efficiently navigate your home and community.
Timeline for Custom Chairs: The entire process, from evaluation to delivery, can take anywhere from 6 to 12 weeks if everything goes smoothly. This timeline depends on the complexity of the chair and the speed of approval from insurance providers and can take up to 6 months at times if there are delays along the way.

Will Medicare Pay for my Wheelchair?
Medicare provides coverage for wheelchairs under its Part B Durable Medical Equipment (DME) benefit, but specific criteria must be met. Most commercial plans also have a DME benefit that is typically based on, or similar to, Medicare standards. Coverage is available when a physician prescribes a wheelchair for use in the home due to a medical condition that limits mobility. Here’s an overview of how this coverage typically works:
Eligibility Requirements: Once you meet with your therapist and vendor team to trial your wheelchair and determine your needs, a physician must then conduct a face-to-face assessment and document the medical necessity of the wheelchair. This documentation is then submitted to Medicare for review.
Types of Wheelchairs Covered: Medicare covers basic manual chairs (rent to own), custom manual chairs, and power wheelchairs if the features are medically justified.
Scooters: Medicare may cover scooters in limited circumstances, such as when mobility is restricted both inside and outside the home, but this coverage is less common.
Costs: For approved devices, Medicare typically covers 80% of the cost, leaving the user responsible for the remaining 20%, either out-of-pocket or through supplemental insurance.
Modification and Replacement: Generally speaking, Medicare expects your custom chair to last at least 5 years. Should your chair require modifications or repair within that five year time frame, you will need to work with your vendor to fix your current chair in most situations. If modifications are required due to a change in your medical status, they may be covered by medicare, but repairs due to wear and tear may be an out of pocket cost. After five years is up, you may be eligible for a new chair should you demonstrate medical necessity for a new chair at that time.

Choosing the right wheelchair is a collaborative process that requires a deep understanding of the individual’s needs and goals. By working closely with a skilled therapist and an experienced vendor, users can find a solution that not only meets their medical requirements but also improves their quality of life. Whether it’s a lightweight manual chair for someone with a spinal cord injury or a custom power chair for postural support, the right match makes all the difference.
At Healthy Aging Physical Therapy, we are proud to offer custom wheelchair assessments in the comfort of your home. This approach can be incredibly beneficial, not only for individuals who may find it difficult to access a clinic but also for tailoring recommendations to fit seamlessly into your living environment. By evaluating how a wheelchair will work within your home - from navigating doorways to accessing essential spaces - we can ensure the best possible outcome for your mobility and independence. If you or someone you know could benefit from an in-home wheelchair assessment, we encourage you to reach out to learn more about how we can help.

May Staff Meeting Updates
May Staff Meeting Update

Did you know that HAPT meets monthly to review patient cases and provide feedback and ideas, as well as for in-services and education? (Ten heads ARE better than one!) As much as I love learning, I love teaching even more, so thought I'd share a few lessons learned with you.
This month we were lucky enough to have two great presentations. First, Dahlia Cohen, Registered Dietician, spoke to us about Nutrition in Parkinson's Disease. We learned that weight management, in particular keeping weight ON, is a big issue for people with Parkinson's Disease. Not only are there changes in taste, swallowing and digestion that can be problematic, but due to the extra movement and muscle resistance that occurs in movement disorders, individuals with PD are often burning way more calories than normal during the day. This creates an energy deficit and this leads to weight loss. How can we help our patients with this problem? Here are a few ideas Dahlia gave us:
Encourage 3 meals a day + 3 Nutrient Dense snacks (like greek yogurt, or nuts).
Make sure to get adequate amounts of protein throughout the day. Your body can only digest about 30 grams at one sitting, so one big steak at dinner won't cut it. Try adding in smaller amounts, more frequently, making sure to time around your meds (levodopa competes with protein for receptor access, so it can make your meds less effective if taken with protein!). Protein is best eaten 30 minutes before taking levadopa or 60-90 minutes after taking meds.
Don't forget your fiber! We need 25-30 grams of fiber/day for optimal digestion and bowel management, and constipation is even more common in PD because gastrointestinal motility is slowed. Adding in green vegetables, whole grains and beans to your daily diet is helpful, and supplementing if needed with something like Metamucil can be helpful when needed.
After we finished learning about what to take in, we talked about 'how it comes out' with our staff PT, Katie Moulison. Katie just finished a great course in Pelvic Health and shared some helpful considerations for working with individuals who may be experiencing incontinence as they age. Here are some helpful take home messages:
Incontinence is common, but not a normal part of aging and there is a lot we can do about it. Wondering if how often you wake at night to 'go' is normal? Normal nocturia (peeing at night) is waking 0-1 times to get up. If it's more often than that, it can disrupt sleep cycles, leave you more tired during the day and lead to increased risk of falls.
Dehydration, constipation and bladder irritants are all common causes of increased frequency, urgency, nocturia and leakage (PS. the acronym FUNL can help you remember what to ask your patients about!).
If you're wondering about your own bladder habits, or trying to help a patient problem-solve their incontinence troubles, start by keeping a Bladder Diary and share it with a pelvic health specialist to get their take. There may be some simple strategies we can try to make it better!
Who are we and where do we go?

Healthy Aging Physical Therapy provides Physical and Occupational Therapy in the comfort of your own home (“Outpatient at Home”). We accept Medicare B, Blue Cross Blue Shield and most Medicare Advantage Plans and provide care in the following communities: Concord, Arlington, Belmont, Lexington, Winchester, Woburn, Stoneham, Melrose, Medford, Malden, Wakefield, Lynnfield, North Reading, Reading, Middleton & Peabody, Massachusetts.