Healthy Aging Physical Therapy Monthly Blog
Understanding Apathy in PD: 10 Ways to Beat Apathy at Its Own Game
Discover why apathy in Parkinson's disease is not laziness, but a neurological symptom that changes how the brain calculates effort and reward. Learn the science behind Parkinson's-related apathy and 10 practical, evidence-informed strategies to overcome it and stay engaged in exercise, social activities, and daily life.
When I think about apathy, I picture my now 15-year-old daughter as a toddler. Back then, whenever I asked her to do something she didn't want to do, her response was almost always the same:
"Don't wanna."
Pick up your toys? Don't wanna.
Put on your shoes? Don't wanna.
Go to dance class and leave mom behind? Definitely don't wanna.
Fortunately, she eventually outgrew that stage. But when I think about apathy in Parkinson's disease, I often think about that same simple response — not because people with Parkinson's are acting like toddlers, and certainly not because they're being stubborn or difficult, but because from the brain's perspective, apathy can sometimes be just that simple.
The Parkinson's brain looks at an activity — even one that is important, meaningful, or enjoyable—and responds with a very quick internal calculation:
"Don't wanna."
The challenging part is that this isn't a response you can always reason with. When we don't understand apathy, we often default to motivational strategies that work for people without Parkinson's disease. We remind people that exercise is good for them. We tell them their physical therapist recommended it. We encourage them to try harder, stay active, or think positively. All of those statements are logical, and all of them may be true. Unfortunately, apathy is not a problem of logic.
Apathy is a neurobiological brain problem - and it is an incredibly common and consistent non-motor symptom of Parkinson’s Disease.
Because of that, apathy can create frustration for everyone involved. Care partners may feel ignored or dismissed. Adult children may worry that their parent is giving up. Healthcare providers can spend months educating someone about exercise, medication management, or healthy habits only to see little follow-through. Meanwhile, the person with Parkinson's often feels guilty, ashamed, or misunderstood because they know what they should be doing but struggle to get started.
The result is that everyone is working hard, but they're working against a barrier they don't fully understand.
The good news is that once we understand the neurobiology behind apathy — what it is, why it happens, and how Parkinson's changes the brain's motivation systems — we can start to work around it instead of against it. Understanding apathy gives us the KEYS to beating apathy at its own game.
What Is Apathy?
Apathy is one of the most common non-motor symptoms of Parkinson's disease, affecting an estimated 20–50% of people living with Parkinson's and becoming more common as the disease progresses. Despite how frequently it occurs, it is also one of the most misunderstood symptoms.
Apathy is often mistaken for laziness, depression, lack of effort, or lack of interest. In reality, it is none of those things.
While depression is characterized by sadness, hopelessness, or loss of pleasure, apathy is primarily a disorder of motivation and initiation. People with apathy often still care deeply about their families, hobbies, health, and future. They may want to exercise, attend social events, participate in therapy, or spend time with friends. The challenge is not that they don't care. The challenge is that turning intention into action has become significantly harder.
One of the most helpful ways to understand apathy is to think of it like a Reward vs. Effort Seesaw.
In a healthy brain, the anticipated reward of an activity generally outweighs the effort required to do it. The brain looks at an activity and thinks, "Going for a walk will feel good," or "I'll enjoy seeing my friends," or "Exercise is worth the effort." The reward side of the seesaw stays high, making it easier to get started.
Parkinson's disease can alter that internal cost-benefit calculation. Researchers increasingly believe that apathy reflects changes within the brain's motivation circuits, many of which rely on dopamine and related neurotransmitter systems. As those circuits change, the brain begins to overestimate effort and underestimate reward. The seesaw flips. Activities that once felt worthwhile now feel burdensome before they've even begun.
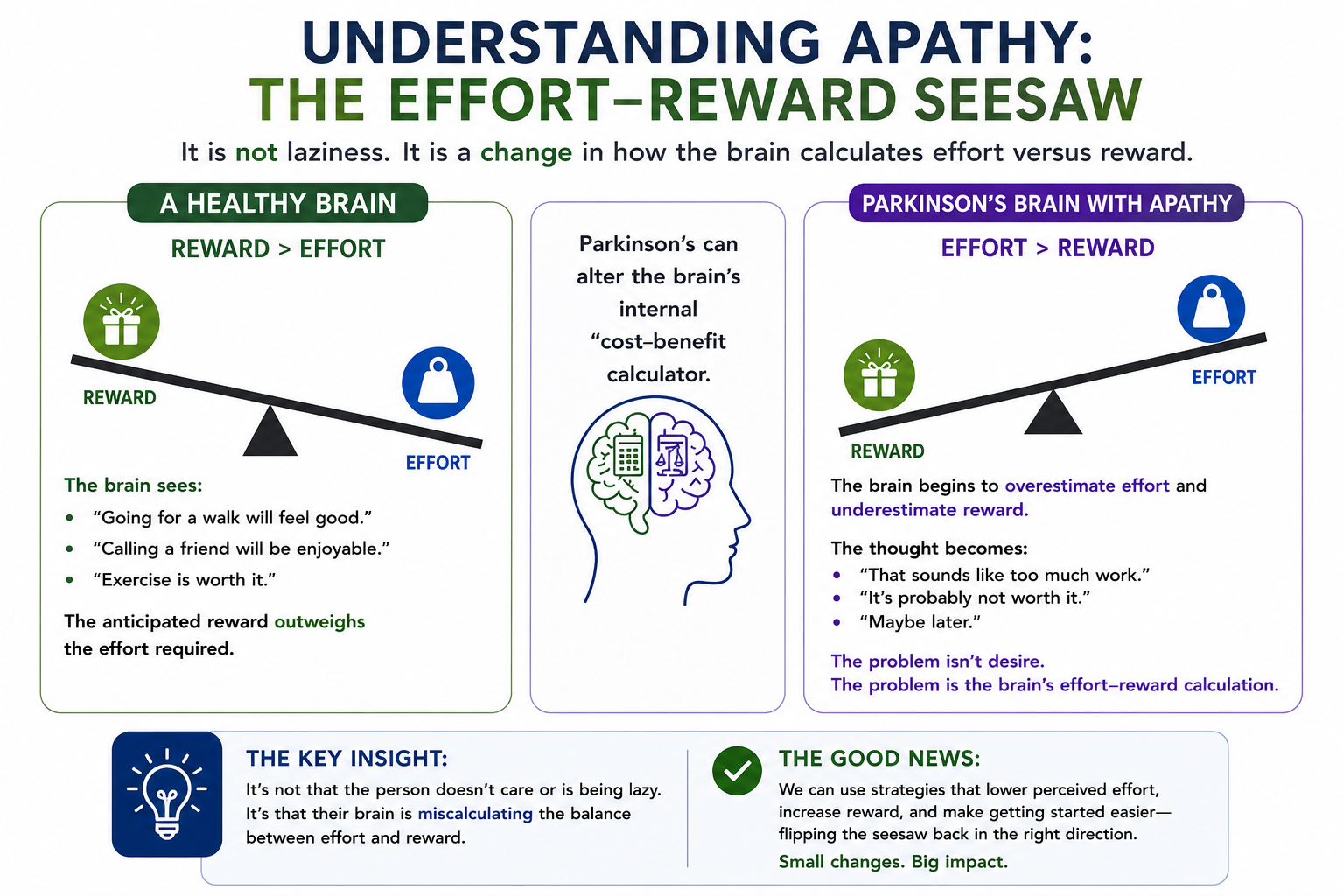
The internal dialogue becomes:
That sounds like a lot of work.
It's probably not worth it.
Maybe later.
Don't wanna.
What's fascinating is that many people with Parkinson's report feeling better after they exercise, attend a class, go for a walk, or meet up with friends. The activity itself wasn't the problem. The challenge was overcoming the brain's initial effort-reward calculation and getting started in the first place.
This understanding is important because it shifts our approach from trying to convince people to be motivated to creating systems that make action easier.
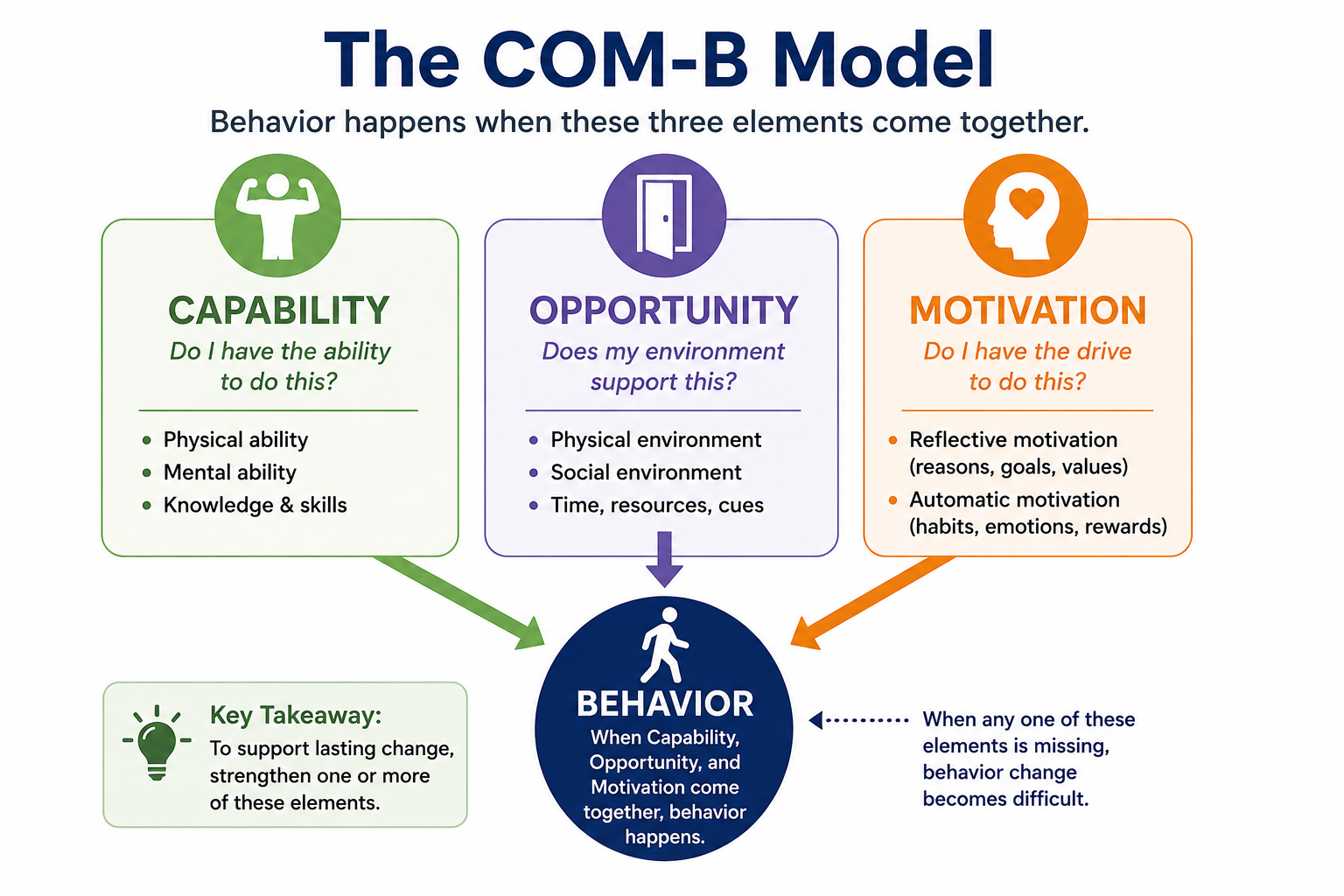
Using the COM-B Model to Outsmart Apathy
One of the most useful behavior-change frameworks discussed at the World Parkinson Congress was the COM-B Model. COM-B proposes that behavior occurs when three things come together:
Capability – Do I have the physical and cognitive ability to do this?
Opportunity – Does my environment support this behavior?
Motivation – Do I have enough drive, reward, habit, or reason to act?
When apathy is present, motivation is often the most obvious barrier, but it's rarely the only one. Sometimes the behavior is physically too difficult. Sometimes the environment creates unnecessary obstacles. Sometimes the reward feels too distant or too small to justify the effort.
The encouraging part is that we don't always have to increase motivation directly. In fact, trying to "motivate" someone with Parkinson's-related apathy is often the least effective approach. Instead, we can change the environment, simplify the task, build routines, leverage social support, and reconnect the activity to something meaningful. We can start to beat apathy at its own game! The following strategies are designed to do exactly that.
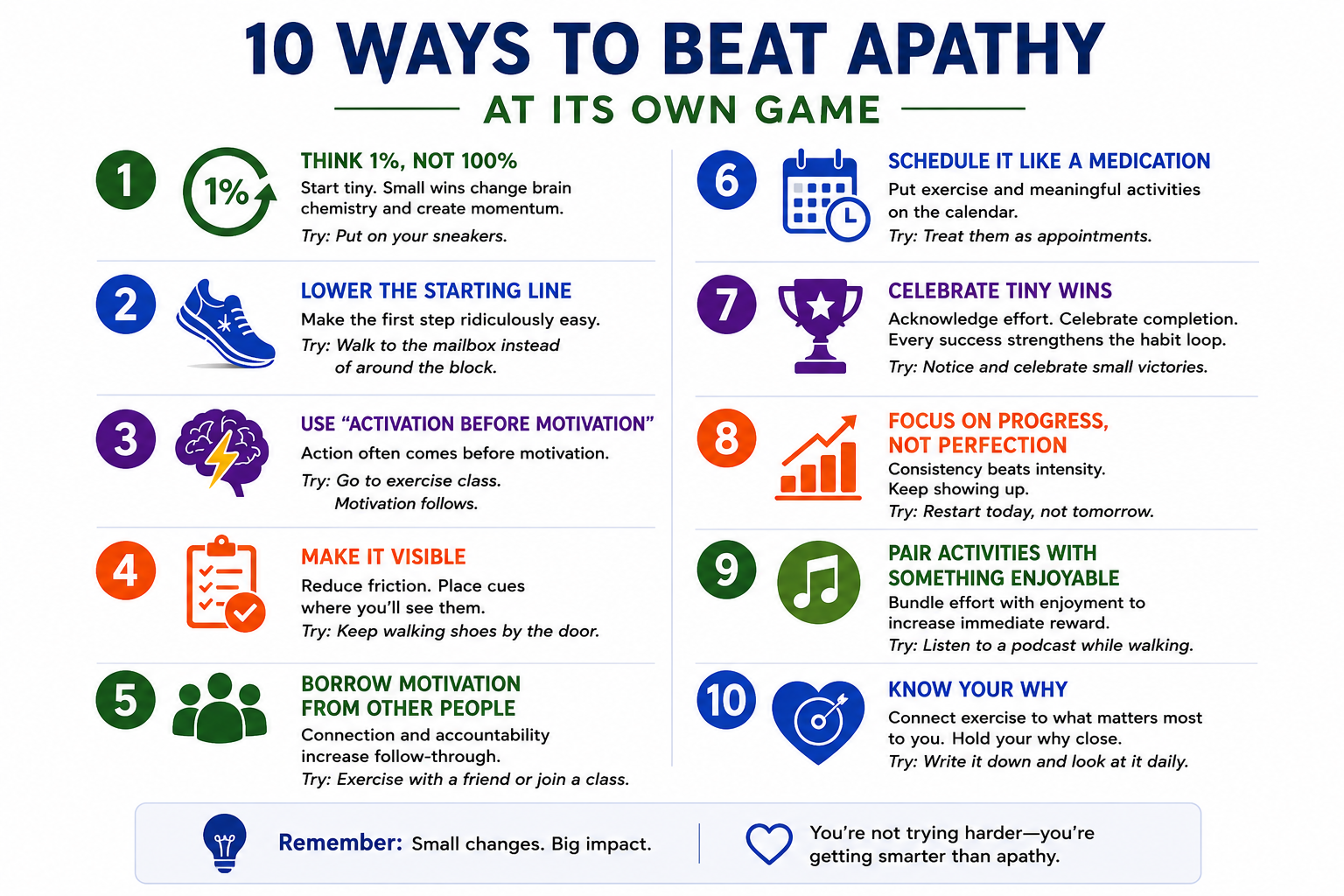
1. Think 1%, Not 100%
One of the most common mistakes people make is trying to change everything at once. Someone who hasn't exercised in months decides they're going to start walking 30 minutes every day. Someone who struggles with household tasks creates a long to-do list. Someone who wants to improve their health commits to changing their entire lifestyle overnight.
The Parkinson's brain often looks at those goals and immediately calculates the effort required. The result is predictable:
"Don't wanna."
Instead of focusing on the final destination, focus on the smallest possible first step. James Clear, author of Atomic Habits, calls this becoming "the type of person who shows up." The goal isn't to complete the workout. The goal is to begin.
For example, instead of committing to a 30-minute walk, commit to putting on your sneakers. Instead of promising yourself you'll complete your entire exercise program, commit to doing one exercise. Instead of attending an hour-long support group, commit to walking through the door. When I go running (which in case you're wondering my brain shouts loudly ‘Don’t wanna!!!), I give myself mini-goals - I’m not out there to run 3 miles, but I am going to run to the next driveway.
The beauty of small actions is that they dramatically reduce perceived effort while creating momentum. Often the hardest part isn't the activity itself—it's getting started.
COM-B Target: Opportunity and Motivation
2. Lower the Starting Line
Closely related to the 1% rule is the idea of lowering the starting line. We tend to believe success comes from raising expectations. In reality, success often comes from making the first step easier.
Many people with Parkinson's create goals that are so ambitious they become intimidating. The brain sees a mountain and decides it would rather stay on the couch.
Lowering the starting line means creating a version of success that feels almost impossible to fail.
If your goal is strength training, perhaps success today is one set of sit-to-stands.
If your goal is walking, perhaps success is walking to the mailbox.
If your goal is exercising three times this week, perhaps success is getting dressed in your exercise clothes and going to check out the local gym or observing a local PD fitness class.
The goal isn't to stay there forever. The goal is to create enough forward momentum that the next step becomes easier.
COM-B Target: Capability and Opportunity
3. Use Activation Before Motivation
Many people believe motivation comes first and action follows, but research suggests the opposite is often true. We wait to feel motivated before exercising. We wait to feel inspired before starting a project. We wait to feel energetic before going out with friends.
The problem is that motivation is unreliable.
Behavioral science consistently shows that action often creates motivation rather than the other way around. Once we begin moving, the brain receives new information. The activity may be enjoyable. We may feel accomplished. We may realize the task wasn't nearly as difficult as anticipated.
For someone with Parkinson's, this is a powerful concept because it shifts the goal from "feel motivated" to "take one action."
You don't have to want to go to exercise class.
You just have to get in the car.
COM-B Target: Motivation
4. Make It Visible
One of the easiest ways to improve follow-through is to redesign your environment.
The more effort required to remember a behavior, the less likely it is to happen. This becomes particularly important in Parkinson's disease, where cognitive load may already be increased. Think about your daily environment.
Do your walking shoes live in the back of a closet?
Are your exercise bands buried in a drawer?
Do you have to search for your water bottle every morning?
Every additional step increases friction.
Instead, place cues where you'll see them. Leave your walking shoes by the door. Keep exercise equipment near your favorite chair. Put your medication organizer somewhere visible. Use calendars, reminders, and visual prompts.
Successful habits often depend less on willpower and more on environment.
COM-B Target: Opportunity
5. Borrow Motivation From Other People
One of the strongest findings in Parkinson's exercise research is that people tend to do better when they're connected to others. Humans are social creatures and we are far more likely to show up when someone else is expecting us.
A walking partner creates accountability.
An exercise class creates routine.
A support group creates connection.
A personal trainer creates structure.
Social support also provides something equally important: encouragement during the inevitable periods when motivation is low. There will be days when you don't feel like exercising. There will be days when symptoms are frustrating. Having people around you who understand those challenges can make all the difference.
Sometimes we don't need more motivation.
Sometimes we just need good company.
COM-B Target: Opportunity and Motivation
6. Schedule It Like a Medication
Most people don't wake up each morning and ask themselves whether they feel motivated to take their medication - They simply do it.
Exercise and meaningful activities deserve the same level of commitment.
One of the most effective strategies for overcoming apathy is removing the decision altogether. Rather than deciding each day whether you'll exercise, decide once and put it on the calendar.
Monday at 10:00 AM.
Wednesday at 10:00 AM.
Friday at 10:00 AM.
Done.
Every decision requires energy. Every decision creates an opportunity for the Parkinson's brain to say "maybe later." Scheduling turns exercise from a choice into a routine.
COM-B Target: Opportunity
7. Celebrate Tiny Wins
The Parkinson's brain can become very good at focusing on what's missing.
"I only walked ten minutes."
"I didn't finish everything."
"I should have done more."
Unfortunately, this mindset reduces reward and reinforces apathy. Behavioral science teaches us that behaviors that get rewarded tend to get repeated. The reward doesn't need to be large. It simply needs to exist.
Did you exercise today? Celebrate it.
Did you attend your support group? Celebrate it.
Did you do one exercise instead of none? Celebrate it.
Your celebration can be a physical ‘air-five’ to yourself, a verbalized ‘You did great today! or a check-off on your tracking worksheet. Progress is progress and repeated acknowledgement of your success will help reset your reward vs. effort seesaw in the proper direction.
Tiny wins create momentum, confidence, and a stronger sense of self-efficacy.
COM-B Target: Motivation
8. Focus on Progress, Not Perfection
Perfectionism can be surprisingly damaging.
When people believe success means doing everything perfectly, they often choose not to start at all.
Missed one workout? The week feels ruined.
Missed a few days? The month feels ruined.
Behavior change doesn't work that way.
The people who succeed long-term aren't the people who never miss a day. They're the people who recover quickly when they do.
One missed workout doesn't matter.
One missed week doesn't matter.
What matters is returning.
Apathy loves all-or-nothing thinking. Progress thrives on flexibility. Instead of letting one missed opportunity derail the next, adopt a ‘next best decision’ mindset and take focus forward, not behind you.
COM-B Target: Motivation
9. Pair Activities With Something Enjoyable
Researchers sometimes call this "temptation bundling."
The idea is simple: combine something you need to do with something you enjoy doing to help increase the immediate reward associated with the activity.
Try listening to your favorite podcast while walking or saving your favorite television show for while you ride your riding the stationary bike.
Make a plan to meet a friend for coffee after exercise class.
The Parkinson's brain often discounts future rewards. Pairing an activity with something enjoyable helps bring some of that reward into the present moment.
COM-B Target: Motivation
10. Know Your Why
This may be the most important strategy of all.
People don't stay motivated because of exercise - they stay motivated because of what exercise allows them to do. If you ask most people why they exercise, most will answer something like ‘I know it’s good for me’ or ‘my doctor said to’ but that's not a why - that's an instruction.
A real why needs to be much more personal.
Maybe it's so you can keep attending your granddaughter's soccer games, or walk on the beach during your annual family vacation.
Maybe it's so you can keep traveling, gardening or playing pickleball with your friends
Maybe it's dancing at a wedding - or being able to walk your daughter down the aisle.
Maybe it's remaining independent and continuing to live in your own home.
THESE are reasons worth fighting for.
When symptoms are challenging and motivation is low, your why becomes an anchor. It reminds you that exercise isn't really about exercise. It's about protecting the life you want to continue living.
Write your why down.
Put it on the refrigerator.
Keep it in your wallet.
Talk about it with your family.
And when the Parkinson's brain says "don't wanna," remind yourself why you started in the first place.
Hold your why tight.
The Bottom Line
Apathy lies.
It tells you the effort is too great. It tells you it isn't worth it. It tells you you'll do it tomorrow, but the science tells a different story.
Most people feel better after they start.
Most people discover the activity wasn't nearly as difficult as their brain predicted.
And most people find that small actions, repeated consistently over time, can create remarkable changes in strength, mobility, confidence, independence, and quality of life.
The goal isn't to overpower apathy through sheer willpower. The goal is to understand how Parkinson's changes the brain's effort vs. reward calculation and then build systems that make action easier.
Start small.
Make it visible.
Use support.
Know your why.
And remember: sometimes beating apathy isn't about trying harder.
It's about outsmarting it and beating it at its own game. And PS: If your brain responded ‘don’t wanna’ after reading all 10 of these tips, it’s because 10 tips is too much right now. Follow the 1% rule and pick ONE TIP and start there. I promise it will help.

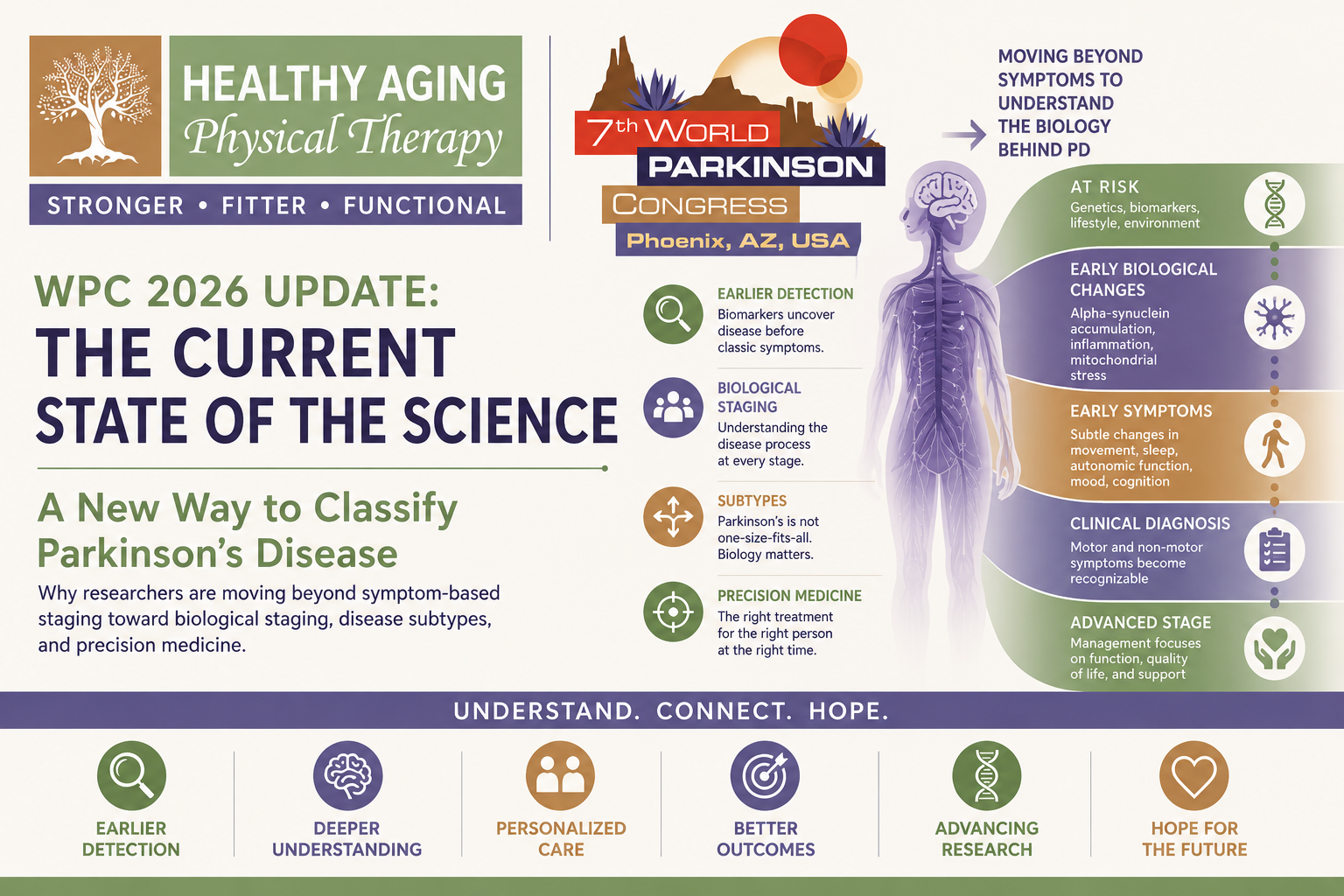
WPC 2026 Update: The Current State of the Science - a New Way to Classify Parkinson’s Disease
Why researchers are moving beyond symptom-based diagnosis toward biological staging systems, disease subtypes, and precision medicine.
Why researchers are moving beyond symptom-based diagnosis toward biological staging systems, disease subtypes, and precision medicine.
One of the most important themes I heard repeatedly at the World Parkinson Congress wasn't about a specific medication, gene, or scientific breakthrough.
It was about something much more fundamental:
How we classify Parkinson's disease.
For decades, Parkinson's disease has largely been diagnosed and staged based on what we can see.
How severe is the tremor?
How much has walking changed?
How much assistance does someone need?
How much disability is present?
Those questions remain incredibly important. But researchers are increasingly recognizing a major limitation:
Two people can look remarkably similar clinically while having very different disease biology.
And two people with very different symptoms may actually share many of the same underlying biological processes.
This realization is driving one of the biggest shifts currently occurring in Parkinson's research—the move from symptom-based classification toward biologic classification.
The Traditional Way We Stage Parkinson's Disease
Historically, clinicians have relied heavily on two major systems.
Hoehn & Yahr Staging
The Hoehn & Yahr scale was first developed in 1967 and remains one of the most widely recognized Parkinson's staging systems.
It focuses primarily on motor symptoms and overall disability.
The stages range from:
Stage 1: Mild, unilateral symptoms
Stage 2: Bilateral involvement
Stage 3: Balance impairment develops
Stage 4: Significant disability but able to walk independently
Stage 5: Wheelchair dependence or need for substantial assistance
The system remains useful because it provides a simple snapshot of disease severity.
However, it has important limitations.
It tells us very little about cognition, sleep, autonomic dysfunction, mood, fatigue, pain, or many of the symptoms that often have the greatest impact on quality of life.
MDS-UPDRS
The Movement Disorder Society-Unified Parkinson's Disease Rating Scale (MDS-UPDRS) provides a much more comprehensive assessment.
It evaluates:
Motor symptoms
Activities of daily living
Non-motor symptoms
Motor complications
The MDS-UPDRS remains the gold standard outcome measure used in both clinical practice and research.
But even this system measures what Parkinson's disease looks like—not necessarily what is happening biologically underneath.
The Problem With Symptom-Based Classification
One of the strongest messages throughout the conference was that symptoms often appear late in the disease process.
Researchers frequently referenced the idea that many people may lose 50% or more of their dopamine-producing neurons before developing recognizable motor symptoms.
If that is true, then traditional staging systems begin measuring disease only after substantial neurodegeneration has already occurred.
Imagine trying to stage heart disease only after someone develops heart failure.
Or trying to stage osteoporosis only after a hip fracture occurs.
That's essentially where Parkinson's disease has historically been.
Researchers are now trying to move the timeline much earlier.
Enter Biological Staging
The field is increasingly shifting toward biologic staging systems that focus on what is happening inside the body before symptoms become obvious.
Rather than asking:
"How severe are the symptoms?"
Researchers are beginning to ask:
"What biological processes are occurring right now?"
This is a fundamentally different way of thinking about Parkinson's disease.
The Alpha-Synuclein Revolution
Much of this shift has been driven by advances in biomarkers.
For the first time, researchers can identify evidence of abnormal alpha-synuclein accumulation in living people through:
Cerebrospinal fluid testing
Skin biopsies
Seed amplification assays
These technologies allow researchers to identify biological evidence of Parkinson's-related pathology before traditional clinical diagnosis in some individuals.
This has created an entirely new framework for thinking about disease progression.
The NSD-ISS Framework
One of the most discussed systems at WPC was the Neuronal Synuclein Disease Integrated Staging System (NSD-ISS).
The goal of NSD-ISS is to create a biologically informed framework that captures disease progression before traditional symptoms appear.
Rather than focusing solely on visible symptoms, the system incorporates:
Alpha-synuclein biomarkers
Genetic risk factors
Early clinical features
Prodromal symptoms
Motor symptoms
The hope is that this will allow researchers to identify individuals much earlier and intervene before significant neurodegeneration occurs.
While still primarily a research tool, many experts believe biologic staging systems will become increasingly important over the next decade.
Why Earlier Staging Matters
The importance of biologic staging becomes obvious when you consider disease-modifying therapies.
Most current experimental treatments are trying to:
Reduce alpha-synuclein accumulation
Improve lysosomal function
Reduce inflammation
Protect mitochondria
Preserve neurons
But these therapies may work best before extensive neuronal loss has occurred.
If researchers can identify people earlier, future treatments may have a much greater chance of altering disease progression.
In other words:
Earlier diagnosis creates earlier opportunities for intervention.
Parkinson's Disease May Not Be One Disease
Perhaps the most fascinating concept discussed at the conference was that Parkinson's disease may actually represent multiple biologic diseases that produce similar symptoms.
This idea is beginning to reshape the field.
Historically, Parkinson's disease has been treated as a single disorder.
Researchers now increasingly suspect that what we call "Parkinson's disease" may actually represent several overlapping biological pathways leading to a similar clinical outcome.
This brings us to the concept of subtyping.
Brain-First vs Body-First Parkinson's Disease
One of the most exciting biologic subtype discussions involved the concept of Brain-First versus Body-First Parkinson's disease.
Brain-First Parkinson's Disease
In this model, pathology appears to begin within the central nervous system.
Alpha-synuclein accumulation may initially occur in structures such as:
Amygdala
Brainstem regions
Central neural networks
Symptoms may emerge differently and biomarkers may follow a unique pattern.
Body-First Parkinson's Disease
In the body-first model, pathology may begin outside the brain.
Potential starting locations include:
Gut nervous system
Autonomic nervous system
Peripheral nervous system
Researchers believe alpha-synuclein pathology may then gradually spread toward the brain.
This model may help explain why some individuals experience years of:
Constipation
REM Sleep Behavior Disorder
Autonomic dysfunction
before motor symptoms appear.
Genetic Subtypes
Researchers are also increasingly identifying biologic subtypes based on genetics.
GBA1 Parkinson's Disease
GBA1-associated Parkinson's disease appears linked to lysosomal dysfunction and impaired protein clearance.
These patients may ultimately benefit from therapies specifically targeting GCase pathways.
LRRK2 Parkinson's Disease
LRRK2-associated Parkinson's disease involves abnormal protein activity that affects cellular maintenance and inflammatory pathways.
Multiple targeted therapies are currently being studied.
Mitochondrial Subtypes
Other forms of Parkinson's disease may involve stronger mitochondrial dysfunction and cellular energy failure.
Researchers continue exploring whether these individuals may respond differently to future therapies.
Clinical Subtypes Still Matter
While biologic subtyping is gaining momentum, clinical subtypes remain important.
Historically, clinicians have classified Parkinson's disease using motor patterns such as:
Tremor-Dominant
Symptoms are driven primarily by tremor.
PIGD-Dominant
Postural Instability and Gait Difficulty (PIGD) symptoms predominate.
However, researchers noted an important limitation.
Up to 50% of individuals may shift motor subtype classifications within only a few years.
These classifications also largely ignore non-motor symptoms.
The Rise of Non-Motor Subtyping
Many researchers now believe non-motor symptoms may provide important clues regarding disease biology.
Potential clinical subtypes include:
Sleep-dominant
Cognitive-dominant
Pain and dystonia-dominant
Autonomic-dominant
Mood-dominant
These classifications better reflect the reality that Parkinson's disease affects far more than movement.
Multiple neurotransmitter systems become involved, including:
Dopamine
Norepinephrine
Serotonin
Cholinergic systems
Autonomic pathways
Sleep and circadian networks
This helps explain why no two people with Parkinson's disease look exactly alike.
The Future: Precision Medicine
All of these changes ultimately point toward one destination:
Precision medicine.
The goal is to move beyond the traditional model where every patient receives essentially the same treatment approach.
Instead, future care may involve identifying:
Disease stage
Biological subtype
Genetic profile
Biomarker status
Dominant disease pathways
and then matching treatments accordingly.
The vision is similar to what has already occurred in cancer care, where biologic testing increasingly guides treatment decisions.
The Bigger Picture
One of the most important things I learned at the World Parkinson Congress is that researchers are no longer asking only:
"Does this person have Parkinson's disease?"
They are increasingly asking:
"What type of Parkinson's disease does this person have?"
That subtle shift may ultimately transform the future of diagnosis, research, and treatment.
For decades we have classified Parkinson's disease primarily by what we could observe.
Today, we are beginning to classify it by what is happening biologically beneath the surface.
And that shift may be one of the most important steps on the road toward earlier diagnosis, better clinical trials, more personalized therapies, and ultimately disease-modifying treatment.
Part 5: The Race Toward Disease-Modifying Therapies
An overview of the most promising approaches currently being tested, including alpha-synuclein therapies, LRRK2 inhibitors, anti-inflammatory treatments, mitochondrial therapies, and innovative platform trials.

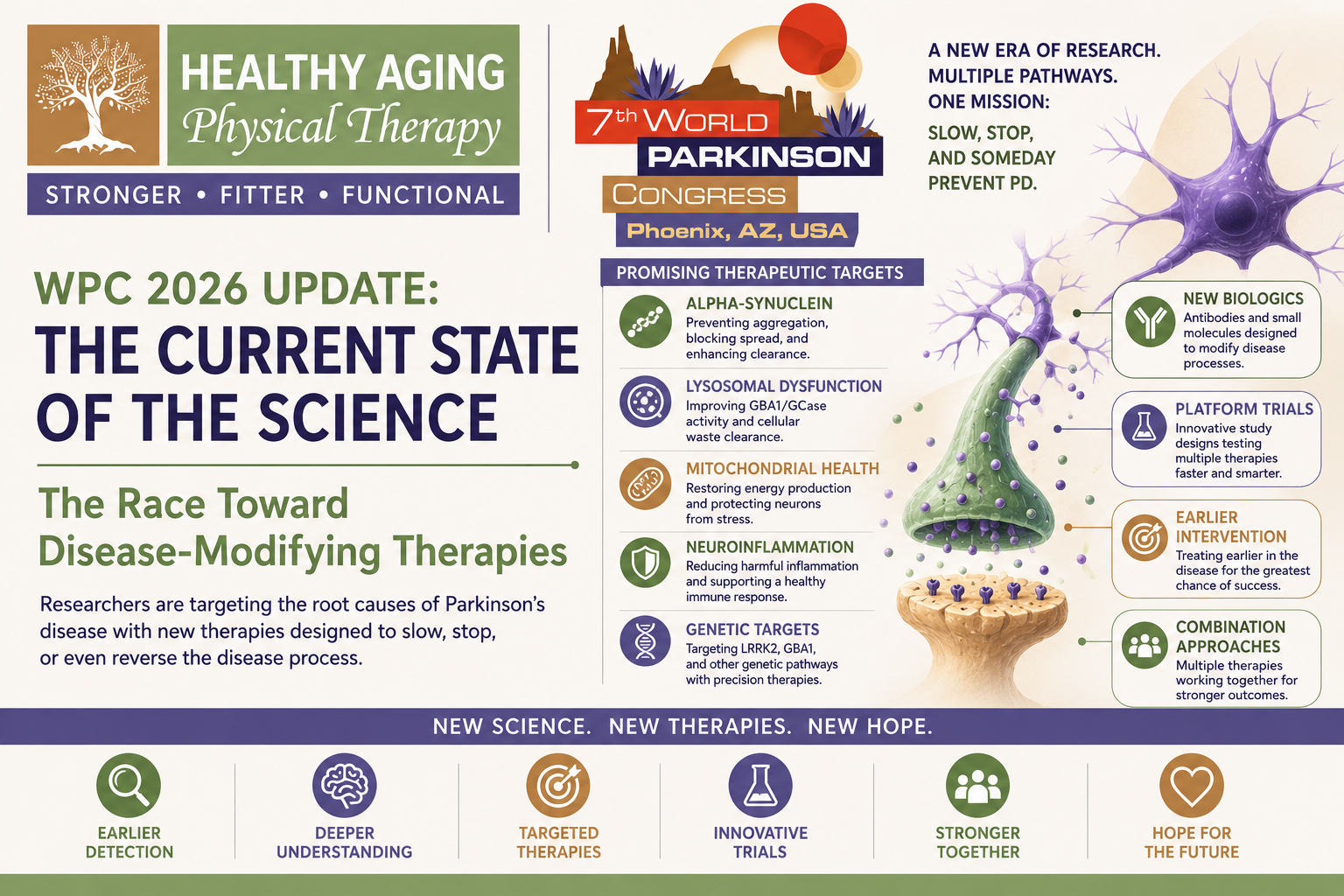
WPC 2026 Update: The Current State of the Science - the Race Toward Disease-Modifying Therapies
From alpha-synuclein antibodies to genetic therapies and platform trials, researchers are pursuing multiple paths toward slowing—or someday stopping—Parkinson's disease progression.
From alpha-synuclein antibodies to genetic therapies and platform trials, researchers are pursuing multiple paths toward slowing—or someday stopping—Parkinson's disease progression.
For decades, Parkinson's disease treatment has focused primarily on managing symptoms.
And to be clear, those treatments have changed countless lives.
Medications like levodopa, dopamine agonists, deep brain stimulation, physical therapy, exercise, speech therapy, and occupational therapy can dramatically improve function and quality of life.
But there has always been one frustrating reality:
None of these treatments have definitively been shown to slow the underlying disease process.
They help people live better with Parkinson's disease.
They do not yet stop Parkinson's disease from progressing.
That is why one of the most exciting themes at the World Parkinson Congress was the growing focus on disease-modifying therapies, often referred to as DMTs.
Rather than simply treating symptoms, disease-modifying therapies aim to slow, alter, or interrupt the biological processes driving Parkinson's disease itself.
In other words, the goal is not simply to help someone move better today.
The goal is to help preserve brain function tomorrow.
Why Has Developing Disease-Modifying Therapies Been So Difficult?
One of the biggest challenges in Parkinson's disease research is timing.
As discussed in previous articles, researchers increasingly believe Parkinson's disease may begin 10–20 years before diagnosis.
By the time tremor, stiffness, slowness, or balance problems become obvious, substantial neuronal loss has often already occurred.
Researchers frequently estimate that 50% or more of dopamine-producing neurons may already be gone by the time symptoms emerge.
This means many therapies may be starting after significant damage has already occurred.
Another challenge is that Parkinson's disease is biologically complex.
There is no single pathway to target.
Instead, researchers are trying to address multiple interacting processes including:
Alpha-synuclein aggregation
Lysosomal dysfunction
Mitochondrial dysfunction
Neuroinflammation
Genetic risk pathways
Cellular energy failure
Impaired protein clearance
The result is a rapidly expanding treatment pipeline that looks very different from what existed even ten years ago.
Target #1: Alpha-Synuclein
If there was one target discussed more than any other at WPC, it was alpha-synuclein.
As we discussed in the previous article, alpha-synuclein is a normal protein that becomes problematic when it misfolds, aggregates, and forms Lewy bodies.
Researchers are pursuing several strategies:
Preventing alpha-synuclein aggregation
Breaking apart existing aggregates
Improving protein clearance
Blocking cell-to-cell spread
Reducing alpha-synuclein production
Prasinezumab
One of the most closely watched therapies is Prasinezumab.
Prasinezumab is a monoclonal antibody designed to bind alpha-synuclein and potentially reduce its spread throughout the nervous system.
Early studies, including the PASADENA trial, did not meet their primary endpoints.
At first glance, this sounds disappointing.
However, longer-term follow-up suggested participants who continued treatment may have experienced slower progression over time.
While far from a definitive success, these findings have kept interest alive and additional studies continue.
One of the strongest messages from researchers was that failed trials do not necessarily mean failed science.
Sometimes they simply mean we have not yet identified the right patients, the right timing, or the right outcome measures.
Target #2: GBA1 & Lysosomal Dysfunction
One of the most promising areas of Parkinson's research focuses on the cell's waste-disposal system.
The GBA1 gene produces an enzyme called glucocerebrosidase (GCase), which helps cells clear damaged proteins and waste products.
When this system becomes impaired, alpha-synuclein may accumulate more easily.
Ambroxol
One of the most exciting therapies currently being studied is Ambroxol.
Originally developed as a cough medication, Ambroxol appears capable of increasing GCase activity and improving lysosomal function.
Researchers hope this will improve protein clearance and reduce alpha-synuclein accumulation.
The ongoing ASPRO-PD Phase 3 trial is evaluating whether these biological effects translate into meaningful clinical benefits.
ACTIVATE Trial
The ACTIVATE study is evaluating Pariceract, a therapy designed to enhance GCase activity.
Unlike many previous studies, ACTIVATE specifically enrolls individuals with GBA1 mutations, representing a move toward precision medicine and targeted treatment approaches.
Target #3: LRRK2
LRRK2 is one of the most important Parkinson's disease genes identified to date.
Researchers believe abnormal LRRK2 activity may contribute to:
Inflammation
Lysosomal dysfunction
Cellular stress
Neuronal injury
The goal of LRRK2 therapies is to reduce excessive activity of the LRRK2 protein.
LUMA Trial
The LUMA trial evaluated a LRRK2 inhibitor in Parkinson's disease.
Although the Phase 2 study did not meet its primary clinical endpoint, researchers successfully demonstrated that the drug reduced LRRK2 activity biologically.
This distinction is important.
Sometimes researchers can confirm they hit the biological target even if they do not yet see the clinical outcomes they hoped for.
Denali & Lighthouse Programs
Additional LRRK2-targeted programs remain ongoing.
These studies continue exploring whether modifying LRRK2 activity can alter disease progression, particularly in individuals carrying LRRK2 mutations.
Target #4: Mitochondrial Dysfunction
Another major theme at WPC was mitochondrial dysfunction.
Mitochondria are the energy generators of cells.
Dopamine-producing neurons require enormous amounts of energy and appear particularly vulnerable when mitochondrial function becomes impaired.
Many researchers now view mitochondrial dysfunction as one of the central drivers of Parkinson's disease progression.
NOPARK Trial
One of the most anticipated mitochondrial studies is the NOPARK trial.
NOPARK is evaluating a nicotinamide-based therapy designed to improve mitochondrial function and cellular energy production.
Researchers hope that supporting mitochondrial health may improve neuronal survival and slow disease progression.
Results are still pending.
Target #5: Neuroinflammation
One of the biggest shifts in Parkinson's disease research over the past decade has been growing recognition of the role of inflammation.
Researchers increasingly believe that immune activation and neuroinflammation may contribute to ongoing neuronal injury.
The challenge is that inflammation is complicated.
Some immune responses may be protective while others may be harmful.
This makes designing anti-inflammatory therapies particularly difficult.
DAPA-PD
The DAPA-PD trial is exploring whether targeting inflammatory pathways can alter disease progression.
Researchers hope to better understand whether reducing harmful inflammation may help preserve neuronal function over time.
This remains one of the most rapidly evolving areas of Parkinson's research.
Why Exercise Keeps Appearing in These Conversations
One of the most fascinating observations from the conference was how often exercise appeared alongside discussions of disease-modifying therapies.
The reason is simple.
Exercise influences nearly every biologic pathway researchers are trying to target pharmacologically.
Exercise has been shown to influence:
Alpha-synuclein biology
Neuroinflammation
Mitochondrial function
Neurotrophic factors
Synaptic plasticity
Cerebral blood flow
Gut microbiome health
Unlike most medications, exercise exerts what researchers call a pleiotropic effect, meaning it affects many biological systems simultaneously.
Several speakers described exercise as the only intervention currently showing consistent evidence of influencing multiple disease pathways at once.
A New Way of Running Clinical Trials
Another exciting topic discussed at WPC was the evolution of clinical trial design itself.
Traditional Parkinson's trials are:
Expensive
Slow
Resource-intensive
Often limited to testing one therapy at a time
Researchers are now adopting innovative approaches designed to accelerate discovery.
Platform Trials
Platform trials allow multiple therapies to be tested simultaneously within the same study infrastructure.
Think of them as clinical trial "hubs" rather than individual stand-alone studies.
This approach allows researchers to:
Test more therapies
Reduce costs
Improve efficiency
Identify promising treatments faster
ACT-PD Platform Trial
One of the most exciting examples is the Edmond J. Safra ACT-PD Platform Trial.
Rather than testing a single therapy, ACT-PD is simultaneously evaluating multiple potential disease-modifying treatments, including:
Telmisartan: Telmisartan is a medication traditionally used to treat high blood pressure, but researchers have become interested in it for Parkinson's disease because of its potential effects on inflammation and brain health.
Telmisartan activates a receptor called PPAR-γ (Peroxisome Proliferator-Activated Receptor Gamma), which plays an important role in regulating inflammation, metabolism, and cellular stress responses.
Researchers believe Telmisartan may:
Reduce harmful neuroinflammation
Protect dopamine-producing neurons from injury
Improve mitochondrial function
Reduce oxidative stress
Support healthy blood vessel function in the brain
Because inflammation is increasingly recognized as one of the major biological drivers of Parkinson's disease progression, Telmisartan is being investigated as a potential disease-modifying therapy rather than simply a blood pressure medication. Researchers are excited because it is already widely prescribed, relatively inexpensive, and has a well-established safety profile.
Terazosin: Terazosin is another medication originally developed for a completely different purpose—treating enlarged prostate (BPH) and high blood pressure.
Researchers became interested in Terazosin after discovering it activates an enzyme called phosphoglycerate kinase-1 (PGK1), which plays a key role in cellular energy production.
This is particularly important because one of the hallmarks of Parkinson's disease is:
Mitochondrial dysfunction
Reduced cellular energy production
Increased vulnerability of dopamine-producing neurons
Terazosin appears to:
Increase glycolysis (the process cells use to generate energy)
Improve ATP production
Support mitochondrial health
Increase cellular resilience under stress
Several observational studies have suggested that people taking Terazosin may experience slower Parkinson's progression compared to those taking similar medications that do not affect cellular energy pathways. Researchers are excited about this one because it directly targets one of the most important biologic themes emerging in Parkinson's disease research: energy failure within vulnerable neurons.
Ursodeoxycholic Acid (UDCA): Ursodeoxycholic Acid (UDCA) is a naturally occurring bile acid that has been used for decades to treat certain liver diseases.
Researchers became interested in UDCA because of its effects on mitochondria.
Mitochondria are often called the "power plants" of cells because they generate the energy needed for survival and function.
In Parkinson's disease, mitochondrial dysfunction is believed to contribute to:
Dopamine neuron death
Oxidative stress
Cellular energy deficits
Increased vulnerability to disease progression
UDCA appears to:
Improve mitochondrial function
Increase energy production
Reduce oxidative stress
Protect neurons from programmed cell death
Improve cellular resilience
Early studies have shown promising signals suggesting improved brain energy metabolism and motor function. Mitochondrial dysfunction appears across many forms of Parkinson's disease—not just genetic subtypes—meaning therapies like UDCA could potentially benefit a broad range of patients.
Istradefylline: Istradefylline is already approved as an adjunct medication for Parkinson's disease in several countries, including the United States.
Unlike most Parkinson's medications, Istradefylline does not work by increasing dopamine.
Instead, it blocks adenosine A2A receptors, which influence activity within the basal ganglia—the brain circuits responsible for movement.
Traditionally, it has been used to reduce "off" time in people taking levodopa.
However, researchers are now investigating whether its effects may extend beyond symptom management.
Potential mechanisms include:
Modulating abnormal basal ganglia signaling
Reducing excessive neural synchrony
Influencing neuroinflammatory pathways
Supporting healthier neural network function
While it is not generally viewed as a classic disease-modifying therapy today, researchers are exploring whether long-term effects on neural circuitry could potentially influence disease progression. This is an interesting approach because it targets a completely different pathway than dopamine and may provide insights into how neural network function contributes to Parkinson's progression.
Overall, this platform approach allows researchers to rapidly identify which therapies deserve larger-scale testing. Plus, if one of these drugs do not reach a successful primary endpoint, they can quickly shift to add another drug to the platform and continue where they left off.
P2P Trial
Researchers also discussed the P2P Trial, another innovative effort designed to accelerate therapeutic discovery through more efficient study designs.
Many experts believe platform trials may dramatically shorten the time required to identify effective therapies.
What About a Cure?
One question inevitably comes up whenever new therapies are discussed:
"Are we getting closer to a cure?"
The honest answer is that we still do not know.
No current therapy has definitively demonstrated the ability to stop or reverse Parkinson's disease.
However, something important has changed.
For the first time, researchers are no longer focused solely on replacing dopamine.
They are actively targeting the biological mechanisms driving disease progression.
That represents a major shift in thinking.
The Bigger Picture
One of the strongest themes throughout the World Parkinson Congress was that Parkinson's research is becoming increasingly biological, increasingly personalized, and increasingly hopeful.
Researchers are no longer searching for a single universal treatment.
Instead, they are targeting multiple pathways simultaneously:
Alpha-synuclein
Lysosomal dysfunction
LRRK2 activity
Mitochondrial dysfunction
Neuroinflammation
Genetic risk factors
The future may not be one disease-modifying therapy.
It may be several.
Just as modern cancer care often combines multiple treatments tailored to an individual's biology, Parkinson's care may eventually move toward personalized combinations of therapies matched to specific disease pathways.
We are not there yet.
But after listening to researchers from around the world discuss the current pipeline, it was impossible not to leave with a sense that the field is moving faster than ever before.
And for the first time in decades, the conversation is no longer just about treating symptoms.
It is increasingly about changing the course of the disease itself.
Part 6: Are We Getting Closer to a Cure?
Exploring stem cells, regenerative medicine, cell replacement therapies, and the realistic possibilities—and limitations—of future curative treatments.
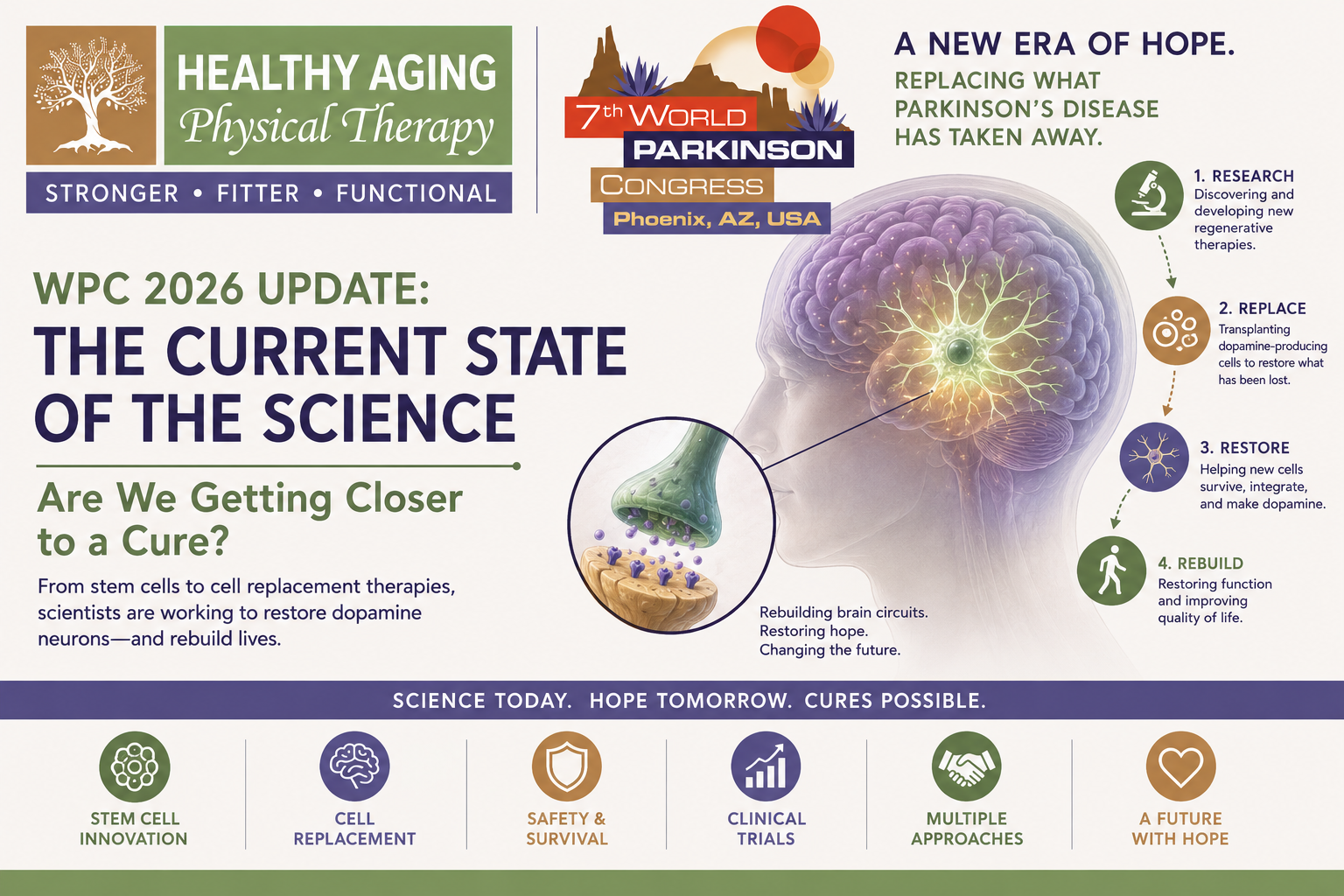
WPC 2026 Update: The Current State of the Science - Are We Getting Closer to a Cure?
Exploring stem cells, regenerative medicine, cell replacement therapies, and the realistic possibilities—and limitations—of future curative treatments.
Exploring stem cells, regenerative medicine, cell replacement therapies, and the realistic possibilities—and limitations—of future curative treatments.
If there was one topic at the World Parkinson Congress that felt the most like science fiction becoming reality, it was regenerative medicine.
For decades, Parkinson's disease treatment has focused on replacing dopamine.
Levodopa replaces dopamine chemically.
Dopamine agonists mimic dopamine's effects.
Deep brain stimulation helps modulate the networks affected by dopamine loss.
These treatments can be incredibly effective. But they all share one important limitation:
They do not replace the dopamine-producing neurons that have been lost.
Regenerative medicine asks a fundamentally different question:
What if we could replace the cells themselves?
Instead of giving the brain dopamine, could we rebuild the brain's ability to produce dopamine on its own?
It sounds almost impossible.
Yet researchers around the world are actively testing exactly that.
The Original Dream
The idea of replacing dopamine-producing neurons is not new.
In fact, scientists have been pursuing some version of this concept for more than three decades.
The rationale is straightforward.
In Parkinson's disease, dopamine-producing neurons within the substantia nigra gradually degenerate.
As these neurons disappear, dopamine levels in the striatum—particularly the putamen—decline.
The putamen plays a critical role in:
Movement initiation
Movement scaling
Motor automaticity
Coordination of movement patterns
Much of the motor disability associated with Parkinson's disease stems from the loss of dopamine input to this region.
Traditional therapies attempt to compensate for that loss.
Cell replacement therapies attempt to restore it.
Early Fetal Cell Transplants
The first major attempts at regenerative therapy involved transplantation of fetal dopamine-producing cells into the brains of people with Parkinson's disease.
Some of the results were remarkable.
A subset of patients demonstrated substantial and long-lasting improvements.
Researchers were able to show that transplanted dopamine neurons could survive, produce dopamine, and integrate into the brain.
For the first time, proof-of-concept existed.
Cell replacement appeared biologically possible.
But there were major problems.
The procedures were difficult to standardize.
Cell quality varied.
Results were inconsistent.
Ethical concerns surrounding fetal tissue limited scalability.
And researchers struggled to reproduce the most dramatic successes consistently.
While the work provided critical insights, it was not a practical path forward for widespread treatment.
The Stem Cell Revolution
Everything changed with advances in stem cell science.
One of the most important breakthroughs discussed at WPC occurred in 2012, when researchers demonstrated that adult cells could be reprogrammed into induced pluripotent stem cells (iPSCs).
This discovery earned the Nobel Prize and fundamentally transformed regenerative medicine.
For the first time, scientists could take ordinary adult cells and essentially rewind them to a stem-cell state.
Those cells could then be guided to develop into dopamine-producing neurons.
This solved one of the biggest obstacles facing earlier transplantation efforts:
Cell supply.
Researchers were no longer dependent on fetal tissue.
Instead, they could generate large numbers of dopamine neuron precursors in the laboratory.
Teaching Cells to Become Dopamine Neurons
Creating stem cells was only the first challenge.
The next challenge was teaching those cells to become the right type of neuron.
Researchers eventually learned that fully mature dopamine neurons often struggled to survive transplantation.
The solution was surprisingly elegant.
Instead of transplanting mature neurons, researchers began transplanting dopamine neuron progenitor cells—cells already committed to becoming dopamine neurons but still capable of adapting and integrating into their new environment.
You can think of them as specialized trainees rather than fully trained workers.
This approach significantly improved survival and integration after transplantation.
The ExPDite Trial
One of the most exciting regenerative medicine studies discussed at WPC was the ExPDite Trial.
This trial uses a stem-cell-derived dopamine neuron progenitor known as Bemdaneprocel.
The goal is straightforward:
Implant dopamine-producing progenitor cells directly into the putamen and allow them to mature into functioning dopamine neurons.
Participants undergo a stereotactic neurosurgical procedure in which tiny burr holes are created and cells are carefully delivered into the targeted brain region.
Because the cells originate from a donor source rather than the patient, participants require approximately one year of immunosuppression to reduce the risk of rejection.
Did It Work?
The most encouraging finding was not symptom improvement.
It was survival.
Researchers demonstrated evidence that transplanted cells survived and integrated into the brain.
That may sound like a small milestone.
It is not.
This represents one of the most important questions regenerative medicine has been trying to answer for decades.
Can transplanted dopamine-producing cells survive inside a human Parkinson's brain?
The answer now appears to be yes.
Researchers also observed improvements in motor function in some participants, although there was considerable variability between individuals.
Importantly, the study met its primary safety goals and did not demonstrate major unexpected safety concerns.
The program has now advanced into Phase 3 clinical trials.
The ASPEN Trial
Another regenerative therapy discussed extensively at WPC was the ASPEN trial.
Unlike ExPDite, ASPEN uses cells derived from the patient's own tissue.
This approach is known as an autologous therapy.
The potential advantages are obvious:
Reduced risk of rejection
Less need for immunosuppression
More personalized treatment
However, there are also challenges.
Every patient's cells must be individually manufactured, processed, and prepared.
This increases complexity, cost, and scalability concerns.
Early ASPEN results have been encouraging, but much larger studies are needed before firm conclusions can be drawn.
Why Regenerative Therapy Is So Exciting
Most disease-modifying therapies aim to slow progression.
Regenerative medicine aims to restore lost function.
That distinction is important.
Researchers often describe regenerative therapy as one of the few approaches capable of potentially rebuilding neural circuitry rather than simply preserving what remains.
If successful, this strategy could fundamentally change how we think about Parkinson's treatment.
Instead of slowing decline, we may someday be able to restore capability.
Why This Is Not Yet a Cure
As exciting as these studies are, researchers were careful to emphasize their limitations.
Replacing dopamine-producing neurons does not necessarily solve every aspect of Parkinson's disease.
Remember the themes we discussed throughout this series.
Parkinson's disease is not simply a dopamine deficiency disorder.
It also involves:
Alpha-synuclein aggregation
Neuroinflammation
Mitochondrial dysfunction
Lysosomal dysfunction
Autonomic nervous system involvement
Sleep and cognitive network changes
Even if cell replacement successfully restores dopamine production, other disease processes may continue.
In other words:
Replacing dopamine neurons may help address one major consequence of Parkinson's disease without necessarily eliminating all of the underlying causes.
The Alpha-Synuclein Problem
One of the biggest unanswered questions involves alpha-synuclein.
Researchers know that alpha-synuclein pathology can spread through the nervous system.
The question becomes:
If new dopamine neurons are transplanted into a brain already affected by Parkinson's disease, what happens over time?
Will those new cells remain healthy?
Or will they eventually develop the same pathology?
Researchers do not yet know the answer.
This remains one of the most important questions in regenerative medicine.
The Most Likely Future
One of the strongest impressions I left the conference with was that the future will probably not involve a single cure.
Instead, it may involve combinations of therapies working together.
Imagine a future where:
Biomarkers identify disease early
Alpha-synuclein therapies slow protein accumulation
Anti-inflammatory therapies reduce neuronal stress
Mitochondrial therapies improve cellular energy production
Exercise supports neuroplasticity and resilience
Regenerative therapies restore lost dopamine neurons
That future looks very different from today's treatment model.
And importantly, pieces of that future are already being tested.
So... Are We Getting Closer?
The honest answer is yes.
Not because a cure is around the corner.
Not because researchers have solved Parkinson's disease.
But because the questions researchers are asking have fundamentally changed.
For decades, the primary focus was replacing dopamine.
Today, researchers are:
Identifying biological subtypes
Detecting disease earlier
Developing disease-modifying therapies
Testing regenerative treatments
Rebuilding neural circuits
Exploring precision medicine
Those are the kinds of questions that eventually lead to transformative breakthroughs.
The Bigger Picture
One of the most hopeful messages from the World Parkinson Congress was that regenerative medicine is no longer theoretical science.
Human clinical trials are underway.
Transplanted dopamine-producing cells have survived.
They have integrated into the brain.
And researchers are beginning to see signals of functional benefit.
Many challenges remain.
Many questions remain unanswered.
But for the first time in history, researchers are not simply asking how to replace dopamine.
They are asking whether we can replace the cells that make it.
And that may be one of the most exciting developments in Parkinson's research today.
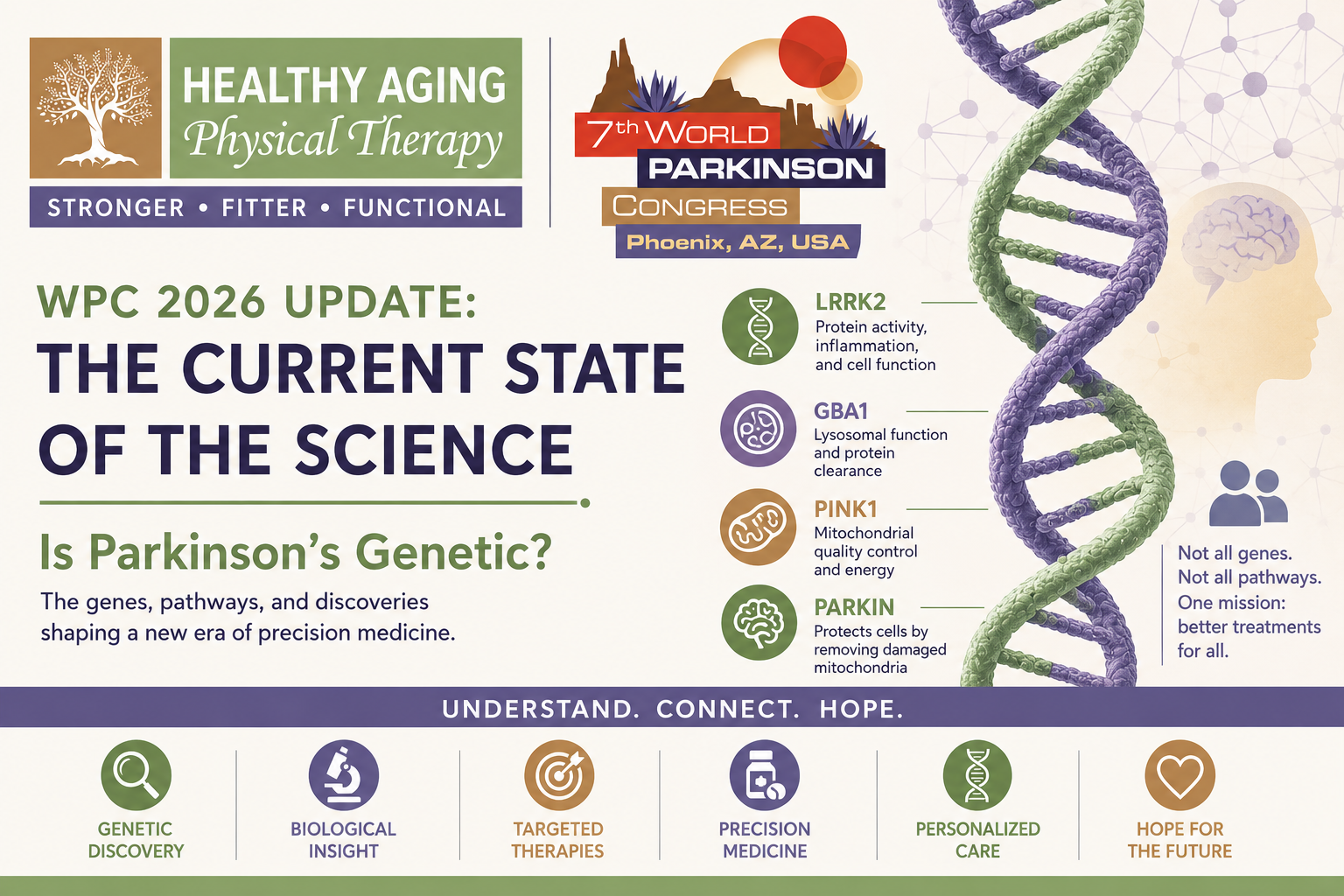
WPC 2026 Update: The Current State of the Science - Is Parkinson’s Genetic?
What scientists have learned about Parkinson's genes, why genetics matters even if you don't have a mutation, and how targeted therapies may help shape the future of treatment.
What scientists have learned about Parkinson's genes, why genetics matters even if you don't have a mutation, and how targeted therapies may help shape the future of treatment.
For many years, when patients asked whether Parkinson's disease was genetic, the answer was often simple:
"Most Parkinson's disease is not inherited."
While that statement isn't entirely wrong, it is becoming increasingly incomplete.
One of the strongest themes I heard repeatedly at the World Parkinson Congress was that genetics is transforming how researchers think about Parkinson's disease. Not because most people with Parkinson's have a genetic mutation—they don't—but because genetics is helping us understand the biological pathways that drive the disease itself.
In fact, some of the most exciting disease-modifying therapies currently being studied were developed because of discoveries made through genetic research.
The question is no longer simply:
"Is Parkinson's genetic?"
The more important question may be:
"What can genetics teach us about why Parkinson's develops in the first place?"
The Short Answer: Sometimes
Most people diagnosed with Parkinson's disease do not have a clearly identifiable inherited genetic mutation.
Researchers estimate that approximately 10–15% of Parkinson's cases have a known genetic component, while the majority are considered "idiopathic," meaning no single cause can be identified.
However, this distinction is becoming less clear.
Even when someone does not carry a known Parkinson's gene mutation, many of the biological pathways affected by genetic forms of Parkinson's appear to be disrupted in idiopathic Parkinson's disease as well.
This means genetic discoveries may ultimately help far more people than just those carrying specific mutations.
The Most Important Parkinson's Genes
Researchers have identified dozens of genes associated with Parkinson's disease risk, but a handful have emerged as particularly important because they appear to influence major biological pathways involved in disease progression.
The genes discussed most frequently throughout the conference included:
LRRK2
GBA1
PINK1
Parkin (PRKN)
Each tells us something different about how Parkinson's disease develops.
LRRK2: The Most Common Genetic Cause of Parkinson's Disease
Mutations in the LRRK2 gene represent the most common known genetic cause of Parkinson's disease.
Approximately 1–2% of all Parkinson's cases worldwide are linked to LRRK2 mutations, though rates are significantly higher in certain populations.
The LRRK2 protein plays important roles in cellular maintenance, lysosomal function, inflammation, and mitochondrial health.
At WPC, one researcher described abnormal LRRK2 activity as being:
"Like a bull in a china shop."
Instead of functioning normally, the mutated protein becomes overactive and may contribute to cellular damage over time.
Because of this, researchers have developed medications designed specifically to reduce LRRK2 activity.
Several major clinical trials are currently evaluating whether suppressing LRRK2 activity can slow disease progression.
While early results have been mixed, the field continues to view LRRK2 as one of the most promising precision medicine targets in Parkinson's disease.
GBA1: The Gene That Changed Everything
If there was one gene repeatedly mentioned throughout the conference, it was GBA1.
GBA1 mutations are among the most common genetic risk factors for Parkinson's disease.
Approximately 5–10% of people with Parkinson's disease carry a GBA1 variant.
The GBA1 gene produces an enzyme called glucocerebrosidase (often shortened to GCase).
This enzyme functions as part of the cell's waste-disposal and recycling system, known as the lysosome.
When GCase activity decreases, cells become less efficient at clearing damaged proteins and cellular debris.
This becomes particularly important because reduced GCase activity is associated with increased alpha-synuclein accumulation.
In other words, one of the major genetic pathways in Parkinson's disease appears directly connected to one of the major protein abnormalities discussed in the previous article.
Even more interesting, researchers now believe many people with idiopathic Parkinson's disease may also have reduced GCase activity despite not carrying a GBA1 mutation.
This is one reason GBA1 research has generated so much excitement.
Ambroxol: From Cough Medicine to Parkinson's Therapy
One of the most discussed GBA1 therapies at WPC was Ambroxol.
Originally developed as a cough medication, Ambroxol appears capable of increasing GCase activity and improving lysosomal function.
Researchers hope that by improving cellular waste disposal, Ambroxol may reduce alpha-synuclein accumulation and slow disease progression.
The ongoing ASPRO-PD Phase 3 trial is currently evaluating whether these biologic effects translate into meaningful clinical benefit.
The fact that a decades-old cough medication is now one of the most closely watched Parkinson's therapies highlights how rapidly the field is evolving.
PINK1 and Parkin: The Mitochondrial Connection
Two additional genes discussed frequently throughout the conference were PINK1 and Parkin.
These genes help regulate mitochondrial quality control.
Mitochondria are often described as the "power plants" of cells because they generate energy needed for cellular survival and function.
Dopamine-producing neurons have exceptionally high energy demands, making them particularly vulnerable to mitochondrial dysfunction.
Under normal circumstances, PINK1 and Parkin work together to identify damaged mitochondria and remove them before they can harm the cell.
When these systems fail, dysfunctional mitochondria accumulate, oxidative stress increases, and neurons become more vulnerable to degeneration.
One of the most important realizations emerging from modern Parkinson's research is that mitochondrial dysfunction appears to occur not only in people with PINK1 or Parkin mutations, but also in many individuals with idiopathic Parkinson's disease.
Again, a genetic discovery has helped uncover a broader biological process affecting many forms of Parkinson's disease.
Why Genetics Matters Even If You Don't Have a Mutation
One of the most important lessons from WPC was that Parkinson's genetics is no longer just about inheritance.
Genetics has become a roadmap for understanding disease biology.
Researchers are increasingly using genetic discoveries to identify:
Biological pathways involved in disease progression
New treatment targets
Potential biomarkers
Distinct Parkinson's subtypes
Precision medicine opportunities
Even if you never undergo genetic testing—or test negative for known mutations—the discoveries coming from genetic research may still influence future treatment options.
The Rise of Precision Medicine
Historically, Parkinson's disease treatment has largely followed a one-size-fits-all model.
Regardless of why someone developed Parkinson's disease, treatment approaches have been relatively similar.
That is beginning to change.
Researchers increasingly believe that Parkinson's disease may consist of multiple biologically distinct subtypes.
Some individuals may have disease driven primarily by alpha-synuclein accumulation.
Others may have stronger lysosomal dysfunction.
Others may demonstrate more prominent mitochondrial abnormalities or inflammatory processes.
This has led to a growing emphasis on precision medicine.
The goal is to match the right treatment to the right patient based on the biological mechanisms driving their disease.
Where Are Genetic Therapies Headed?
Many of today's most promising disease-modifying therapy trials are directly tied to genetic discoveries.
Researchers are currently investigating:
LRRK2 inhibitors
GBA1-targeted therapies
Lysosomal enhancers
Mitochondrial therapies
Gene therapies
RNA-based therapies
Precision medicine approaches guided by biomarkers and genetic testing
Some studies have produced encouraging results.
Others have failed to meet their primary endpoints.
But as several researchers emphasized throughout the conference, failed trials often teach us as much as successful ones.
The field continues to move forward rapidly.
The Bigger Picture
The most exciting thing about Parkinson's genetics may not be identifying who inherited a mutation.
It may be what those mutations are teaching us about the disease itself.
Genes such as LRRK2, GBA1, PINK1, and Parkin have opened windows into critical biological processes including protein clearance, mitochondrial health, inflammation, and cellular waste management.
These discoveries are helping researchers move beyond simply treating symptoms and toward therapies designed to address the underlying biology of Parkinson's disease.
And perhaps most importantly, they are helping reshape how we think about Parkinson's itself.
Rather than one disease with one cause and one treatment, Parkinson's increasingly appears to be a collection of overlapping biological pathways that may require different approaches for different people.
That shift—from symptom management toward biologically targeted precision medicine—may ultimately become one of the most important advances in Parkinson's research over the next decade.
Part 4: The New Way We Classify Parkinson's Disease
Why researchers are moving beyond symptom-based diagnosis toward biological staging systems, disease subtypes, and precision medicine.